This article will be a continually updated log for my injectable SARMs cycle and review of injectable LGD-4033 (Magnalone).
Rather than publish a separate article for each update, I will come back and update this article accordingly with any blood work or new findings.
For those that are just here find out where to buy injectable SARMs, this is the company I used for this log:
Swiss Chems – 25% off coupon code “DC25”
This is another company I have experimented with for injectable SR9009, injectable L-Carnitine and some other miscellaneous products:
Amino Asylum – 20% off coupon code “DC20”
The Goal Of This Experiment
In my log introduction I outlined the goal of this experiment.
My goal of this experiment was to truly evaluate how anabolic injectable SARMs are without any interfering factors.
To be more specific, I wanted to find out if injectable LGD-4033 could “replace” a TRT dose of Testosterone entirely in a muscle growth/retention context.
If injectable SARMs could replicate the same muscle building potential as traditionally used anabolic steroids with a fraction of the androgenic activity, the potential applications would be endless.
LGD-4033 is purported to have a 500:1 anabolic to androgenic ratio.
The following graph illustrates the data derived from the preclinical studies which exhibits how much LGD-4033 stimulated muscle growth relative to prostate growth in comparison to Testosterone.
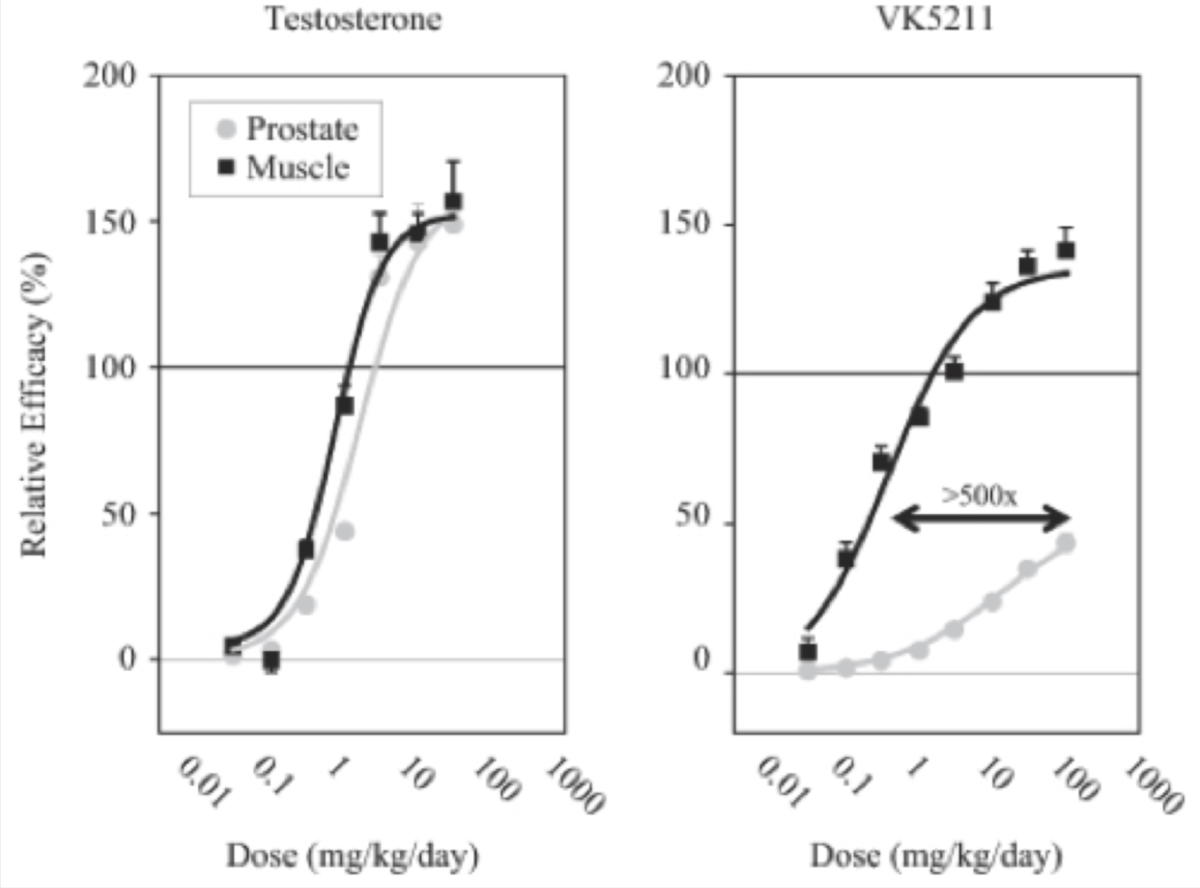
LGD-4033 stacked up against Testosterone very well in the preclinical models with a greater than 500x tissue selectivity of muscle to prostate.
As LGD-4033 is so tissue selective, individuals who are extremely prone to the androgenic side effects of Testosterone may be able to utilize LGD-4033 as a way to build supraphysiological amounts of muscle mass, or retain it, with a relative absence of those same side effects.
How I Determined Exactly How Anabolic Injectable LGD-4033 Is By Utilizing Exogenous Estradiol
Most guys using injectable SARMs are using them alongside a Testosterone base at minimum.
To truly evaluate the efficacy of injectable LGD-4033 in an anabolism context, all other androgens would need to be removed from the equation.
As I just finished a Nandrolone monotherapy experiment prior to starting LGD-4033, my endogenous androgen production was completely shutdown.
Estrogen is what has shown to be neuroprotective and not Testosterone (and potentially cardioprotective as well).
Estrogen also supports several other functions in the body that would be inhibited if I were to forgo Estrogen replacement during this experiment.
These include but are not limited to muscle growth and fat loss.
I needed to isolate LGD-4033 and keep myself shut down to accurately assess how anabolic it is, so adding an exogenous aromatizing compound was not an option.
The most common solution to insufficient Estrogen would be a Testosterone base, DHEA, HCG, or an aromatizing anabolic steroid like Dianabol or Trestolone to act as a makeshift “Test base”.
None of these were viable options as they would add anabolic and androgenic activity to my body and skew my findings.
The only option was to utilize exogenous Estradiol at a physiologic dose.
This is because exogenous Estradiol would prevent my natural Testosterone production from turning back on (endogenous Testosterone production would also skew my findings), it would activate Estrogen receptors sufficiently to bandaid the issue of insufficient aromatization to fulfill physiologic functions, and it would not elevate androgenic activity in the body at all.
In theory, by maintaining a physiologic level of Estrogen in the body I could largely avert the inhibition of anabolic pathways and assess exactly how anabolic LGD-4033 is with no factors interfering.
The only potential drawback here is that aromatase is what normally regulates Estrogen production endogenously, and by bypassing this process entirely I could very well be missing out on some downstream anabolic pathways that would otherwise be fulfilled by Testosterone aromatizing into Estrogen.
Just one of these being the IGF-1 pathway.
The experiment is not perfect, but it is the closest I am going to get to it.
Prior to my Nandrolone experiment I was maintaining my physique on 100 mg of Testosterone per week, and I was able to retain the same level of muscle mass and strength during my Nandrolone experiment with no other factors changed.
If injectable LGD-4033 proved capable of maintaining my physique with no factors changed in my diet or training, then I would know that it is at least as anabolic as Testosterone and Nandrolone, but with a fraction of the androgenic activity.
Oral SARMs Vs. Injectable SARMs
Oral SARMs have shown to have a handful of common side effects in a clinical setting, with numerous other side effects cropping up when utilized in a performance enhancing context at higher dosages.
The main side effects that are consistently seen both clinically as well as anecdotally with oral SARMs are:
- Negative Effect On Lipid Profile
- Natural Testosterone Suppression
- Liver Toxicity (less common)
Other less common side effects start to crop up once the dosage used greatly exceeds what has been evaluated on humans clinically.
The potential benefits that injectable SARMs have over oral SARMs mainly come down to increased bioavailability and skipping the first pass effect in the body after administration.
Bioavailability
Many SARMs have undisclosed oral bioavailability and are presumed to be low based on the lack of published data.
Obviously this isn’t a scientific way to go about determining a SARM’s oral bioavailability, but until these pharmaceutical companies start to release more transparent data, researchers will speculate and make assumptions that could be true, or could be way off.
Some SARMs have shown to have reasonable levels of oral bioavailability, but we don’t have exact figures for the majority of them.
The closer a SARM is to 100% the closer it is to complete absorption after oral dosing.
With injection, complete bioavailability is guaranteed as we are basically forcing the body to assimilate it into the blood and carry it to target tissues, whereas with oral administration we are giving the body’s oral drug metabolism an opportunity to break down the compound however it sees fit.
By ensuring complete bioavailability with injection, we may be able to minimize the dosage required to yield a desired effect.
In theory, this should result in less side effects and more anabolic activity milligram for milligram.
This is the first potential benefit of injectable SARMs over oral SARMs.
In some cases, like with SR9009 (not a SARM but is commonly lumped into the “SARMs” category), the body nearly completely breaks it down when it is administered orally, rendering it ineffective.
Some oral SARMs are very bioavailable as is and we do have the data to reinforce that.
For example, the SARM S23 is 96% orally bioavailable [R].
This means that S23 can be administered orally, as opposed to requiring injections to achieve maximal blood serum concentration levels, which is obviously advantageous when it comes to ease of use and adoption.
The First Pass Effect – Drug Metabolism
Despite having nearly 100% bioavailability, oral S23 administration may have a completely different effect in the body simply by injecting it.
The same could apply for any other SARM too, not just S23.
After a drug is swallowed, the digestive system absorbs it and it enters the hepatic portal system.
Afterwards, the portal vein carries it into the liver for metabolization, which then essentially regulates how much is filtered out prior to delivery to the circulatory system for delivery to target tissues.
Not only can this process greatly reduce how much of a drug actually gets through for utilization, but it can produce a variety of side effects that wouldn’t occur with methods of administration that skip the first pass.
Methods of administration like transdermal delivery or injection skip the first pass and can avoid the hepatotoxicity often associated with oral drug metabolism, as well as other side effects that can stem from the drug metabolism process itself.
More often than not, this is a good thing.
However, in the case of anabolic agents, it seems that the first pass can actually be responsbile for the potentiation of certain compounds, rather than the other way around.
You can see how this can start to make injectable SARMs vs. oral SARMs murky territory, as we basically need to experiment with it ourselves to see if the increased bioavailability and skipping the first pass improves the anabolic activity relative to the side effect profile of SARMs, or makes it worse.
For what it is worth, as of now the results seem promising, with the majority of individuals noting only drastically increased levels of anabolic activity at lower dosages, and less side effects.
However, regardless of how promising and exciting this may seem, we need to consider the possibility of negative outcomes and not let the hype around injectable SARMs shroud our judgment.
Examples Of How The First Pass Effect Can Greatly Impact Drug Effects
The following are two examples of how drastic of a difference just changing the method of administration can have when it comes to a drug’s effects on the body.
The first shows how injectable and transdermal estradiol was superior to oral estradiol, and the second shows how oral Superdrol was superior to injectable Superdrol (in a tissue selectivity context, not a hepatotoxicity or lipid dysfunction context).
Oral Estrogen Vs. Transdermal Or Injectable Estrogen
A few of the most notable drawbacks of oral estrogen pills are that they can be somewhat liver toxic, they significantly spike SHBG levels, and they result in the production of clotting factors in the blood that do not develop with forms of administration that skip the first pass.
Also, the ratio of Estrone-to-Estradiol is skewed with massive elevations in Estrone with oral Estrogen administration.
None of these issues occur with transdermal topical application, or injection.
High levels of serum Estrone sulfate (E1S) were found after long-term oral estrogen treatment of commonly prescribed dosages, whereas there was a small increase in E1S levels after transdermal Estradiol (E2) therapy.
The mean maximum E1S levels were more than 20-fold higher with oral estradiol (E2) when compared with the 0.05 mg/day transdermal estradiol patch.
This is consistent with the 20-fold higher dose of E2 when compared with the transdermal dose [R].
Oral estrogen also has very low bioavailability, thus requiring a much higher dosage to achieve the same effect that could be achieved with a much lower dosage of injectable estrogen.
Oral Superdrol Vs. Injectable Superdrol
Not only is the side effect profile of oral Superdrol compared to injectable Superdrol substantially different, but even its anabolic to androgenic ratio changes based on the method of administration.
When administered orally, Superdrol was more anabolic than methyltestosterone and several times less androgenic than methyltestosterone.
Methyltestosterone has an anabolic to androgenic ratio similar to that of testosterone (close to 1:1).
When administered via injection, Superdrol was nearly twice as anabolic as testosterone and twice as androgenic as testosterone.
The results of subsequent assays to determine Superdrol’s anabolic and androgenic activity found that that Superdrol possessed the oral bioavailability of methyltestosterone while being 400% as anabolic and 20% as androgenic, yielding an anabolic to androgenic ratio of 20:1 [R].
In the case of Superdrol, injecting it actually made it less tissue selective, despite oral administration having the obvious drawback of lower bioavailability and hepatotoxicity.
My Daily Injectable LGD-4033 And Estradiol Dosage
As the goal of this experiment was to determine the lowest effective dose of LGD-4033 that could replicate the same anabolic activity as 100 mg of Testosterone per week and 100 mg of Nandrolone per week, my dose was much lower than what most are utilizing in their own experiments.
Once I could determine the lowest effective dosage, I could evaluate the side effect profile of that dosage, how my blood work looks on that dose, how I feel, and then make an informed decision about the overall efficacy profile of injectable LGD-4033 based on all of those factors.
As injectable LGD-4033 is more bioavailable, the dosage required to replicate the anabolic activity I was shooting for would likely be much lower than you would expect via oral dosing.
I spoke to Tony and Trevor about this experiment and asked for their feedback on what dose they think I should start at.
They were the two who brought injectable SARMs to my attention in the first place, and nobody else I know had any experience with them at the time.
At 7:02 in the following video Tony and Trevor are referring to me, and that is partially what influenced my decision to go with 3 mg per day as my daily dose.
I also applied 2.5 grams of transdermal Estrogel (delivering 1.5 mg Estradiol) per day for the first couple weeks.
I got my blood test results back from my Nandrolone experiment a couple weeks into my LGD-4033 experiment which showed that I was absorbing Estrogel very poorly, which prompted me to switch to oral Estradiol pills.
My dose was 1 mg per day of Estrofem (oral 17ß-oestradiol).
Ideally I would have switched to Estradiol injections, but I did not have any injectable Estradiol on hand, so I was forced to use oral pills if I wanted to maintain an optimal Estradiol level throughout the experiment.
Injectable LGD-4033 Half-Life And Dosing Schedule
Orally, LGD-4033 displayed a prolonged elimination half-life (24–36 hours), linear pharmacokinetics, and predictable accumulation with multiple dosing [R].

There was a dose-proportional increase in LGD-4033 concentrations on days 1 and 21 because of its long half-life.
Serum LGD-4033 concentrations were nearly threefold higher on day 21 than on day 1, reflecting accumulation upon multiple dosing.
There is not any human data we can refer to that evaluates the pharmacokinetics of injectable LGD-4033, so any statements made about how often it should be dosed are largely based on speculation and educated guesses.
Tony and Trevor believe that injectable LGD-4033 can be dosed every other day and still maintain stable blood serum concentrations.
For the sake of ensuring stability once dose saturation was reached, I maintained a daily dosing schedule from day 1 where I administered 3 mg every 24 hours.
Muscle Growth And Strength Levels
How I assess if something is working or not is by comparing it to my previous baseline metrics I have established on a therapeutic dose of TRT.
If I suddenly start getting stronger while using the exact same diet and training regimen with the only factor changed being a drug, I can logically conclude that the drug is stronger milligram for milligram than my baseline on TRT.
By now, I know exactly how my body responds to 100 mg of Testosterone per week, as well as 100 mg of Nandrolone per week.
After swapping to injectable LGD-4033 with no other factors changed, it was very easy to assess if there were any positive or negative changes in my body composition or strength.
Other than feeling a bit deflated, I didn’t experience any changes in my strength or size.
My weight stayed exactly the same, my strength stayed exactly the same, and my body composition stayed the same, with the exception of being a bit flatter.
Perhaps the reason I’m flatter is that LGD-4033 has less “off target” activation than something like Testosterone and Nandrolone, whereby they can increase intramuscular fullness via indirect mechanisms.
That is just speculation though.
At the end of the day, I haven’t lost any contractile tissue, which is the most important thing to note.
I believe that a relatively low dose of injectable LGD-4033 is at least as anabolic as 100 mg of Testosterone per week or 100 mg of Nandrolone per week.
While this is promising for those on TRT or who use “low” dosages of anabolic steroids, the main drawback we have seen in the past with oral SARMs is that the ceiling where diminishing returns starts to set in is far lower than with anabolic steroids.
Whether or not injectable LGD-4033 has that same drawback remains to be seen.
Anecdotally, other users have reported that the ceiling of diminishing returns is much higher with injectable LGD-4033, but I cannot confirm or deny this myself as that is beyond the scope of my experiment (at least for now).
My only hope for this experiment was that I could retain all my muscle with just a SARM, which I did.
I may consider a “blast” phase in the future where I titrate the dose up and evaluate how well it can support supraphysiological muscle growth, but that will be dictated by its androgenicity in practical application.
Injectable LGD-4033’s androgenicity still needs to be explored more via further experimentation, as I did have a few red flags of androgenic activity that have me a bit hesitant to utilize a higher dose.
If injectable LGD-4033 is as tissue selective as the clinical data has shown, there are several doors that open up in a bodybuilding and hair loss prevention context.
Side Effects
Changes In Libido
My sex drive went up substantially after swapping Nandrolone out for LGD-4033.
Many were quick to comment on my YouTube video about how exogenous Estradiol (E2) is the reason why my libido spiked.
I was already on exogenous Estradiol prior to the injectable LGD-4033 for my Nandrolone-only experiment.
I have been on the same dose of transdermal E2 for almost 3 months, the only thing that changed was swapping NPP out for LGD.
The libido change was from the swap.
No other factors were changed.
After I switched from transdermal Estradiol to oral Estradiol, my libido was no different either.
The change in libido occurred almost overnight after adding LGD-4033 in.
Several other individuals have come forward since that video was published reporting that injectable LGD-4033 increased their libido as well.
They were all using a dose at least 5-10x higher than I was, but it is still notable nonetheless.
As LGD-4033 is supposed to be so tissue selective and have such a lack of androgenicity I was very surprised that my libido spiked.
If anything, I was expecting my libido to drop.
With a 500:1 anabolic to androgenic ratio, obviously you wouldn’t expect one of the biggest red flags of androgenic activity to spike.
Keep in mind, 100 mg of Nandrolone per week is not nothing.
Despite Nandrolone being one of the least androgenic steroids ever developed (if not the least of the mainstream anabolic steroids), 100 mg per week has shown to be a high enough dose to cause virilization in women.
Within 12 weeks, some women will experience virilization on Nandrolone even using only 100 mg every 2 weeks.
When duration of use exceeds a year, significant virilization in women is found even at a dosage of only 50 mg every 2 weeks.
My libido doubled after switching from NPP to injectable LGD-4033, which is a red flag and should be noted.
My libido isn’t as high as it is on 100 mg per week of Testosterone, but it is significantly higher than on Nandrolone.
Hair Loss
I noticed an increase in shedding using injectable LGD-4033.
Further experimentation will be needed before I have a concrete conclusion on the androgenicity of injectable LGD-4033.
If it ends up being hair safe, there are several applications I have in mind for this compound.
Not only would it be a potent androgen receptor agonist for use in a bodybuilding context, but it could also be utilized during a hair recovery phase.
For example, if you have any androgenic alopecia, periodically switching to SARMs with exogenous Estradiol (or an Estrogen precursor) in cycles could be a way to maintain muscle built via supraphysiological steroid use in the past, while reducing the androgen load on the scalp significantly enough to allow for regrowth.
Or, if you don’t use steroids, it could serve as a means of recovering hair lost via endogenous androgen induced miniaturization by reducing androgenicity below baseline periodically throughout the year.
Basically like a makeshift anti-androgen that won’t strip the muscle off your body.
These are hypothetical examples, but these are just a few of the potential applications I see for SARMs in the future.
*Update February 26th, 2020*
I do not believe injectable LGD-4033 at the dosage I used is hair safe, and it may be even worse than some traditional AAS (see my blood work results video below for more elaborate details).
Changes In Body Hair Growth
This one was a metric I should have kept a closer eye on, but I usually manscape every single week so it wasn’t something I originally planned on evaluating.
A few weeks into my LGD-4033 experiment I noticed that my body hair seemed to be growing a bit faster than usual.
Whether this was in my head or not, I’m not positive as I was not even planning on using this as a metric, but I got backlogged on work throughout the holidays and ended up skipping my weekly manscaping sessions.
While it may not be fair to say for certain that LGD-4033 increased my rate of body hair growth, I can confidently say that at the absolute least, it did not reduce my body hair growth.
This is notable as well because I had no androgens in my body.
If I only had Estrogen in my system and no androgens I would notice a drastic reduction in body hair growth and libido, just like transgenders who transition from male to female.
The only anabolic compound in my body throughout this entire experiment was injectable LGD-4033, and I didn’t notice a reduction in androgenic activity via body hair growth either.
When I crushed my DHT levels to 0 with Dutasteride, I noticed a significant reduction in back hair growth.
On injectable LGD-4033, I did not notice a reduction in body hair growth at all.
However, on Nandrolone I did not experience a significant reduction in body hair growth either, despite it dramatically reducing my libido.
While this metric isn’t a scientific way to assess androgenic activity, in general, the body can tell you pretty accurately when androgenic activity is high or low when sufficient Estrogen is present to support erections.
Increase the androgenic activity in your body and you will likely experience an increase in libido, an increase in scalp hair loss, and an increase in body hair growth (in general).
Decrease the androgenic activity in your body and you will likely experience a decrease in libido, a decrease in scalp hair loss, and a decrease in body hair growth (in general).
Changes In Blood Pressure


My blood pressure on injectable LGD-4033 is identical to what it is normally on TRT.
My blood pressure on injectable LGD-4033 and TRT is far better than it is on Nandrolone.
For whatever reason, Nandrolone has a unique negative impact on systolic blood pressure, making it difficult to maintain healthy levels.
On only 100 mg of NPP per week my systolic blood pressure was consistently 125-128 eating the exact same diet I was on TRT and LGD-4033.
So far so good in regards to blood pressure on injectable LGD-4033 though.
Changes In Resting Heart Rate


My resting heart rate did not increase on injectable LGD-4033 and is no different than what it is on TRT.
Potential In Preventing Or Reversing Cardiovascular Issues Caused By Steroid Use
Even if injectable LGD-4033 does not end up being as purely anabolic as we hoped, there is another very promising application I see for injectable SARMs that is largely overlooked.
That is the potential lack of heart stimulation.
Anecdotally, many users have reported far better outcomes using SARMs than anabolic steroids in a cardiovascular health context.
One example is a friend of mine, Alek Mitrevski.
He used 100 mg of oral S4 (Andarine) with 0.5 mg oral Estradiol per day for over a year straight.
During that time he did not experience any cardiac hypertrophy, LVH, or any kind of deleterious effect on his cardiovascular system.
At the start of 2019 Alek ran a high dose Deca only cycle with Anadrol intermittently added in.
Within 9 months, he experienced significant thickening and enlargement of his heart.
He switched back to SARMs only to try and reverse this damage while maintaining the muscle he built with the Deca + Anadrol blast.
Although the reports are obscure and not well documented, I have seen a handful of individuals report the reversal of cardiomyopathy and LVH after switching to SARMs only.
SARMs are supposed to be tissue selective, whereas anabolic steroids have shown to significantly impair cardiac health.
The potential applications this may have for athletes seeking supraphysiological muscle growth with a minimization of cardiac hypertrophy, LVH, etc. makes injectable SARMs worth further exploration in itself.
Athletes seeking to reverse cardiovascular issues as a result of past AAS abuse while maintaining most (or all) of their hard earned muscle mass would also be strong candidates for benefiting from injectable SARMs if the hype around them turns out to be justified.
My Blood Test Results
*Update February 26th, 2020*
I got my blood test results and I am adding them to the article now here:
My commentary is also available in the video, but to put it simply, the blood test results were disappointing and I will be ending the experiment now.
Reviews From Other Users
I have curated all of the injectable LGD-4033 reviews I could find and included them here for your reference as well.


















The following comments weren’t reviews about injectable LGD-4033 specifically, but they were relevant to include nonetheless:






Conclusion
Some of the classic signs of androgenic activity are red flags worth keeping an eye on.
But other than that, so far so good.
I feel good, I am not depressed and have not experienced any negative mental or physical side effects so far despite the near complete absence of Testosterone and DHT in my body.
The fact that injectable LGD-4033 has proved capable of maintaining the same amount of muscle and strength that I could maintain on 100 mg of Testosterone per week and 100 mg of Nandrolone per week is a good sign.
I was hoping for that outcome, and expecting more than that is wishful thinking.
If a relatively low dose of injectable SARMs can replicate the same anabolic activity of traditionally used steroids, then it is absolutely worth further experimentation.
I’m going to continue digging into injectable SARMs, and I look forward to seeing more data come from other researchers in the community as well.
This is a very promising area of research, and I hope that more individuals start to come forward with their personal findings too.
I’ll keep you guys updated, but that is where we’re at with my injectable SARMs experiment so far.
*Update February 26th 2020*
My blood test results came back, and I have some concluding thoughts on this experiment I highly recommend you listen to thoroughly prior to any experimentation of your own.
Where To Buy Injectable SARMs
I strongly advise that before you buy SARMs from a company online you thoroughly evaluate their track record, their third party test results, and how they are marketing their products in general.

Disclaimer: The information included in this article is intended for entertainment and informational purposes only. It is not intended nor implied to be a substitute for professional medical advice. Prior to buying anything, check that it is compliant where you live with your current government laws.