In this article I detail what I wish somebody taught me before I started using anabolics about the ideal testosterone dosage to use during a bulking phase.
When I first got into bodybuilding, I started researching bodybuilding pharmacology like a maniac.
I was on the forums daily, I would rack the brains of guys I considered veterans in the community, I would listen to gurus, and I would scour the internet for anything I could find.
For the last decade I’ve been absorbing information, and filtering out the crap.
As you’ve probably experienced first hand, there is A LOT of garbage that circulates in this community.
Unfortunately, when I first started researching there weren’t nearly as many credible sources of information in the community.
The logical conclusion you make as a newbie is that the guy who is older and bigger than you probably knows more than you, so you should probably take what they say as solid advice.
I did this a lot, and I also took a lot of theories to heart that weren’t backed with any science.
With that being said, personal experience is still very important.
A research paper can only tell you so many things about X compound before you need to just try it for yourself to really have valuable insight on its potential benefits and drawbacks in a bodybuilding context.
My personal experience and research has led me to many conclusions that I wouldn’t have been able to wrap my head around even a few years ago, let alone when I first started learning about this stuff.
The Point Of Using A Testosterone Base
One of the most misunderstood concepts in our community is the Testosterone base.
I had heard for years that Testosterone needs to be a base for every single steroid cycle.
No matter what, you needed to have Testosterone in there.
Logically, this makes sense on the surface.
We naturally produce Testosterone, so if you shut down your hypothalamic–pituitary–gonadal axis (HPG axis) with exogenous steroids then you would need to replace your Testosterone production with exogenous Testosterone.
That was as far as anyone would explain the point of a Test base though, and for several years I accepted that as best practice.
At a higher level, despite the fact that a Test base is still something that will be beneficial for the vast majority of AAS users, it is important to understand why you are injecting a steroid to begin with.
Why exactly is an oral-only cycle a poor choice at a higher level than your gym bro telling you “if you don’t use Test you will get f*cked up!”
Well, the main reason you need Testosterone is not just to activate androgen receptors and transcribe anabolic and androgenic effects in tissues in the body, but also it is to aromatize into a sufficient amount of Estrogen to fulfill a myriad of other physiological functions.
Only in recent years has the importance of adequate Estrogen levels been highlighted even by experts in the community, and the previous dogma in the community up until the last few years was that Estrogen is bad and you should use an Aromatase Inhibitor to lower Estrogen to the middle of the reference range no matter what.
Little consideration was given for the androgen to Estrogen ratio in the body, the fat loss and growth factor inhibiting effect unnecessarily lowering Estrogen can have, or the massive impact Estrogen has on lipid modulation.
The clinical data also suggests how neuroprotective and cardioprotective Testosterone is relative to other anabolic steroids, but often fails to acknowledge that this effect may not be mediated by Testosterone at all, rather, it is the Estrogen that is created as a result of aromatization in the body.
Give a man a bunch of any drug that suppresses Testosterone production to nearly zero and you will see a subsequent spike in neurotoxicity and cardiotoxicity.
Creating a therapeutic amount of Estradiol in your body is mediated through Testosterone aromatizing into Estrogen.
While there are synthetic steroids that have proven to act on Estrogen receptors, or aromatize into Estrogen themselves, they have inherent flaws that cannot match the bioidentical androgen our body modulates in all aspects with far greater ease.
- Dianabol aromatizes into 17α-methylestradiol and is inherently hepatotoxic.
- Equipoise (Boldenone) is a poor substrate for aromatase and is incredibly kidney toxic relative to Testosterone.
- Trestolone aromatizes into 7α-methylestradiol and could potentially become a viable “test base” alternative, but for the time being, its therapeutic efficacy in this context still lags behind the obvious go to which is bioidentical Testosterone.
- Nandrolone is a very poor substrate for aromatase and will not maintain healthy levels of Estradiol relative to the androgen load exerted on the body, even at high dosages.
While certain steroids can activate Estrogen receptors or aromatize into Estrogens themselves, none fit the bill for a perfect balancing act in all aspects like bioidentical Testosterone does.
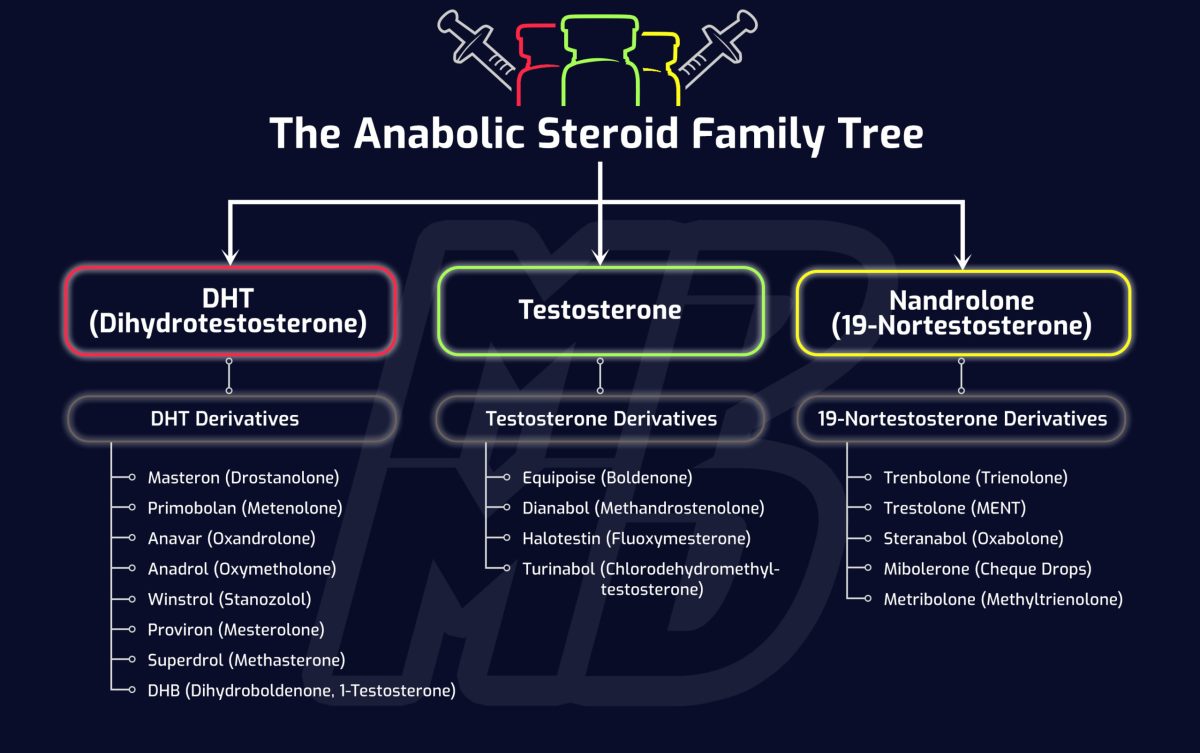
The 3 Categories Of Steroids
The anabolic steroids we use for bodybuilding more or less break down into 3 different categories that you should understand thoroughly.
Testosterone (and its derivatives), DHT Derivatives, and 19-Nor’s.


Testosterone And Its Derivatives
The main steroids we concern ourselves with in this category include Testosterone, Dianabol and Equipoise.
Aside from Trestolone, these are the only notable steroids that provide enough Estrogenic activity to function as “bases” of a cycle.
DHT Derivatives
The main steroids we concern ourselves with in this category include Masteron, Proviron, Winstrol, Primobolan, Anavar, Anadrol and Superdrol.
DHT derivatives are not substrates for aromatase and thus have minimal estrogenic activity (with the exception of Anadrol).
19-Nortestosterone (Nandrolone) Derivatives
The main steroids we concern ourselves with in this category include Nandrolone, Trenbolone and Trestolone (MENT).
The Point Of Stacking Other Anabolics With Testosterone
The main purpose of the Testosterone base is to maintain a physiologic amount of Estrogen that you would otherwise lose when your endocrine system is shut down in the presence of exogenous androgens.
Once this function is fulfilled and you have that therapeutic level of Estradiol (E2) fulfilled via a base of Testosterone, what are you doing above and beyond that that’s helping you in a bodybuilding context?
When I was first getting into my research I would commonly see 500 mg of Testosterone per week being deemed a “newbie cycle” dosage, and a Test base during a cycle was no less than 500 mg per week in every single cycle thereafter when stacked alongside other compounds.
The dosage of Testosterone proposed in the “ideal” newbie cycle is so high that you already have guys on their first cycle forced to use Aromatase Inhibitors to prevent Estrogenic side effects.
In general, if you need to use an aromatase inhibitor to use a certain dosage of Testosterone, I would deem that dosage of Testosterone too high for you.
Testosterone is a great muscle building hormone, but oftentimes there are better ways to get the job done with lower overall stress on the body.
Remember, Testosterone is one of the most primitive steroids there is.
All steroids developed after Testosterone were synthesized in attempts to make a more tissue selective hormone than Testosterone in order to be used in a clinical setting with higher levels of tolerability.
Tolerability, virilization, and health/biomarker impact are three very different metrics to assess the overall safety profile of a compound.
The ideal anabolic agent would induce a significant amount of anabolic activity, with a relative lack of impact on biomarkers and masculinization.
This is easier said than done though.
This is what drove chemists to continue synthesizing new steroids after discovering Testosterone.
You can’t inject a woman with a bunch of Testosterone to prevent muscle wasting without inducing severe virilizing side effects.
Expectedly, more tissue selective alternatives that can induce the same anabolic activity with less side effects are more ideal in a therapeutic setting.
This is also why the development of SARMs is very promising.
This is where compounds like Primobolan, Anavar and Nandrolone showed such therapeutic promise too.
With that being said, anabolic/androgenic ratios aren’t the end all be all that we should base our compound choices on, and oftentimes they are completely incorrect (e.g. with Winstrol).
When To Stack Other Steroids With Testosterone
Taking this all into consideration, if muscle growth with a minimization of negative health impact is the goal, this is what I would suggest.
After ensuring you have a physiologic amount of testosterone as your base at minimum, would it be wiser to increase your Testosterone dosage into the stratosphere and force yourself to introduce adjunct ancillary drugs to continue breaking plateaus, or introduce anabolic steroids that complement your base.
Well, that depends on your genetic propensity to aromatization among numerous factors, but in general, I would say that the most intelligent approach to creating a steroid cycle should be increasing Testosterone as much as you can get away with until the need for an aromatase inhibitor presents itself.
Obviously I’m not suggesting you do this on a first cycle, or perhaps even a second or third cycle, but I’m trying to lay out a framework to determine when/if it is justified for you to start stacking on top of your base.
As long as Testosterone dosages are slowly tapered upwards as you gain muscle mass, side effects can be kept to a minimum with greater ease than most other compounds.
The exception to this are androgenic side effects, but for the sake of this article being focused on bodybuilding outcomes and health, I will be disregarding hair loss/androgenic side effects when I lay out this framework.
The synergy between Testosterone and more tissue selective alternatives will always give better results on a milligram for milligram basis, but the impact that total milligram amount per week has on your health, and other things you may or may not care about (e.g. your hair) is what you need to take into consideration.
Testosterone wins over all other compounds when you factor in everything with exception of androgenic side effects, but there comes a point for the majority of individuals where more Testosterone is just not feasible without forcing the user to introduce an AI.
For those who can blast Test into the sky with no side effects, frankly, they’d probably be better off using a slowly titrating dose of Testosterone to continue breaking plateaus with all things considered (finances, bloodwork, long term health ramifications, etc.).
But, for those who are very prone to estrogenic side effects, stacking will be necessary if your goals in muscle accrual exceed what you can accomplish with a moderate dosage of Testosterone.
Testosterone will produce dose-dependent increases in muscle mass.
We already know this.
However, once you hit a certain dose (individual dependent), you will be forced to introduce adjunct drugs just to mitigate side effects, which will also impair other important biomarkers and hinder muscle growth.
This dosage is typically around the 300-400 mg Testosterone per week mark for many individuals.
If you don’t need an AI though and your body is extremely efficient at balancing androgens relative to estrogens, then by all means, push the Testosterone higher instead without stacking if your biomarkers indicate that it is the healthier choice for you.
Testosterone has proven time and time again to be the most forgiving steroid on health markers and it is more than sufficient to grow a physique to IFBB pro standards.
Pharmaceutical grade Testosterone is also relatively easy to find for a fair price, whereas pharmaceutical grade Primobolan, Anavar, Nandrolone and Anadrol are commonly faked, or very expensive.
How To Know What Compounds To Choose In Your Stack
Once you get to a point where you’re forced to use an AI just to use a higher dose of Testosterone, was it a wise choice to use that much Testosterone in the first place?
Personally, I believe that is where introducing a DHT derivative would then be justified rather than increasing your Testosterone dosage even higher.
The DHT derivative will accomplish the following:
- Exhibits inherent anabolic effects itself and are typically well tolerated (several DHT derivatives are decent muscle builders).
- Some can bind with SHBG, consequently freeing up more Testosterone to be used in tissues. Thus making your current dose of Testosterone work “better”.
- Some can antagonize Estrogen, consequently reducing your need for an AI. This may even give you more wiggle room to increase your Testosterone dose even higher without needing an AI.
Only once you’ve plateaued from a cycle comprised of a Test base and a DHT derivative do I believe you should even consider introducing a 19-Nor, as they are the least forgiving on health markers, despite their superior anabolic/androgenic tissue selectivity.
All steroids accomplish the same thing at the end of the day more or less, so how they are used in your protocol should be based on your propensity to side effects and individual specific biomarkers.
In addition, your tolerance to androgenic activity needs to be factored in, as managing hair loss and other androgenic side effects on hormones is a totally different ballgame than managing side effects in a completely health focused context.
While you can get to 260+ pounds lean on a bunch of Testosterone (if you have great genetics), could you have not accomplished the same thing with a much lower androgen load, or without needing to pop AI’s like candy to tolerate the dosage of Testosterone needed to support that much lean muscle growth?
This is what I wish I learned about sooner, because it wasn’t until after I finished trying to chase bodybuilding goals that I feel I really started to understand more optimal practices.
Misconceptions Surrounding Certain Compounds
Certain compounds that are very effective get completely overlooked because of their relative lack of potency, and oftentimes even their relative lack of side effects.
“Wet” compounds like Dbol will give the user an inflated look as a result of its conversion to 17α-methylestradiol.
If something bloats you up 10 pounds nearly overnight, does that mean it is a more effective muscle builder than something dry but less dramatic due to its relative lack of side effects?
No, I don’t think so.
Compounds like Primobolan will get overlooked because of this, and they are seen as “girl steroids”.
If you’re in this for the long haul, long term muscle growth is our goal with the least impact on our health possible.
There are very few compounds that edge out Primobolan in this regard, despite yielding what may be perceived to be better increases in size in the short term.
The reality is, there are several commonly overlooked compounds with better outcomes than commonly reached for steroids not only in a clinical setting, but in a bodybuilding context as well in the long-term.
Comparing someone waterlogged on a Test, Nandrolone and Dbol cycle to someone on a Test, Primobolan and Nandrolone cycle, the guy on Dbol might appear to be making significantly more progress at a much faster rate, but are those outcomes just inflated by the guy being waterlogged?
Or are they actually yielding more nitrogen retention and lean muscle accrual with their inclusion of Dbol?
The side effect profile of the second cycle would be far more tolerable and still yield nearly identical gains in muscle mass all things considered.
Keep this in mind when you’re designing your cycles.
How I Would Approach A Blast Phase
If somebody outlined these concepts to me when I was younger I could have significantly reduced my dosages and avoided so much unnecessary hair loss, cardiovascular stress, oxidative stress, and organ stress in general.
My dosages were excessive for my goals was the main issue, which I outline further in my article detailing my first cycle.
If I were to design subsequent blast phases for myself now (and hair loss wasn’t a concern), it would follow the framework I outlined earlier in the article.
Testosterone Dosage
I would use a base of 300 mg Testosterone per week split into everyday administrations.
My Testosterone dosage would titrate up to as high as my body can tolerate without needing an AI or substantial detriment to my health markers during the subsequent cycle.
DHT Derivatives
Primobolan
In the subsequent cycle I would introduce a DHT derivative like Primobolan if I hit a wall with my titrating Testosterone dosage.
By hit a wall, I mean that I am put in a position where I need more AAS, but increasing my Testosterone dosage any further would result in me needing to introduce an AI to prevent significant estrogenic side effects from occurring.
So, instead of increasing Testosterone further and using an AI, at that point we can look to the DHT derivative family.
The dosage of Primobolan would titrate up as needed based on SHBG and Free Testosterone levels (Primo doesn’t bind well to SHBG, but the dosage would still be based on what my limits are with Testosterone titration), estrogenic activity in the body, biomarkers, and my tolerability of 19-Nor’s.
19-Nortestosterone (Nandrolone) Derivatives
Nandrolone
Nandrolone is my choice of 19-Nor that would be introduced several cycles later once my body had plateaued from all of the previous blast phases where I had already peaked my Test base dosage and tried a subsequent cycle of a Test base with Primobolan.
Advanced AAS Protocol Framework
The foundation of each blast phase after I deem my body had reached an “advanced” stage of AAS use again would likely include Testosterone as my base, Primobolan and Nandrolone.
While certain compounds could be considered interchangeable, I see no need to rotate compounds in and out during a mass building phase.
The primary growth promoters of that stack are Testosterone and Nandrolone, but the dosages of each would be highly dependent on individual gene expression and health markers (as well as basic things like blood pressure).
I’ve been on therapeutic TRT for years so I would milk this compound progression again if I wanted to experience significant progress without needing to jump straight into an advanced stack.
It should take you at least a couple years of cycling before you work your body up to a point where a protocol designed using advanced cycle framework is even necessary to deploy to break muscle building plateaus.