Muscle Chemistry Archive
Injectable SARMs Review – LGD-4033 (Magnalone)
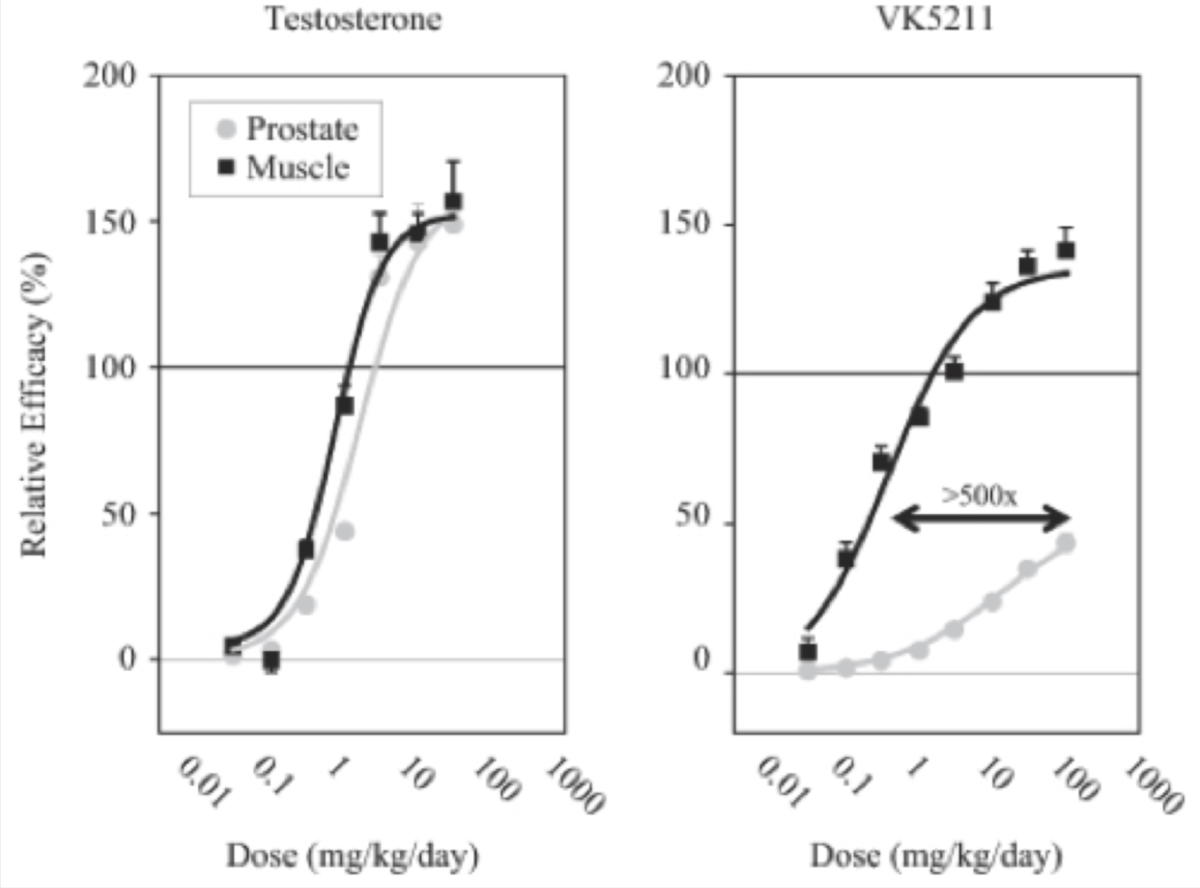
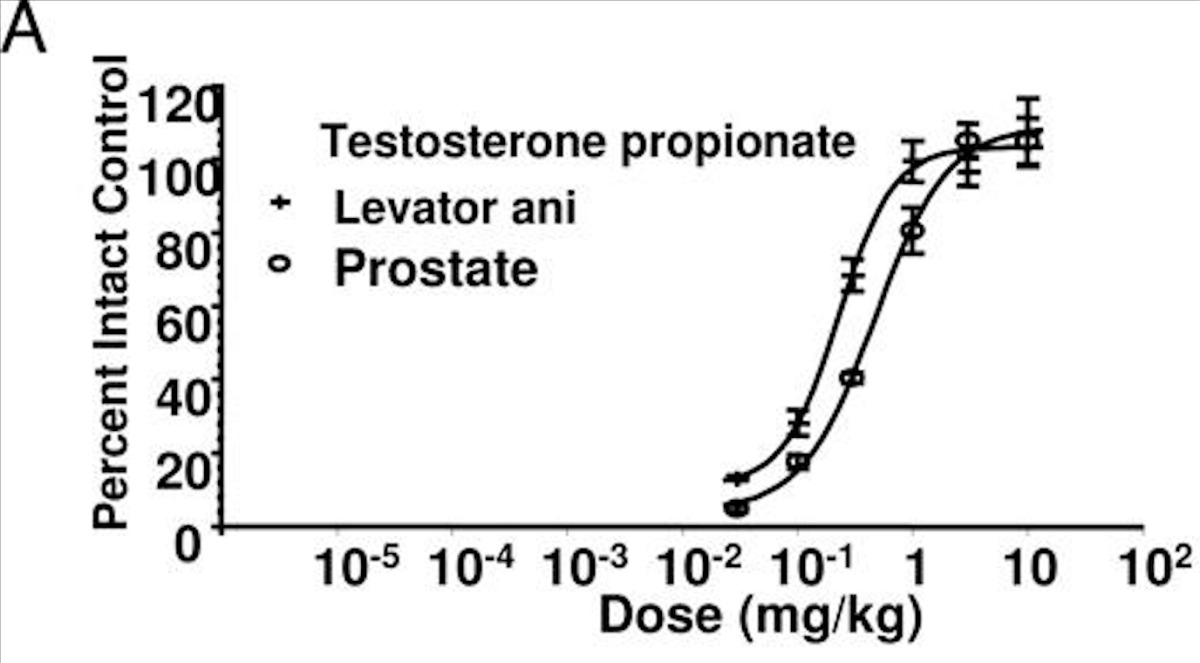
This article will be a continually updated log for my injectable SARMs cycle and review of injectable LGD-4033 (Magnalone).Rather than publish a separate article for each update, I will come back and update this article accordingly with any blood work or new findings.For those that are just here find out where to buy injectable SARMs, this is the company I used for this log:Swiss Chems – 25% off coupon code “DC25”This is another company I have experimented with for injectable SR9009, injectable L-Carnitine and some other miscellaneous products:Amino Asylum – 20% off coupon code “DC20”Table of ContentsThe Goal Of This ExperimentIn my log introduction I outlined the goal of this experiment.[embedded content]My goal of this experiment was to truly evaluate how anabolic injectable SARMs are without any interfering factors.To be more specific, I wanted to find out if injectable LGD-4033 could “replace” a TRT dose of Testosterone entirely in a muscle growth/retention context.If injectable SARMs could replicate the same muscle building potential as traditionally used anabolic steroids with a fraction of the androgenic activity, the potential applications would be endless.LGD-4033 is purported to have a 500:1 anabolic to androgenic ratio.The following graph illustrates the data derived from the preclinical studies which exhibits how much LGD-4033 stimulated muscle growth relative to prostate growth in comparison to Testosterone.LGD-4033 Selectivity For Muscle To Prostate Compared To TestosteroneLGD-4033 stacked up against Testosterone very well in the preclinical models with a greater than 500x tissue selectivity of muscle to prostate.As LGD-4033 is so tissue selective, individuals who are extremely prone to the androgenic side effects of Testosterone may be able to utilize LGD-4033 as a way to build supraphysiological amounts of muscle mass, or retain it, with a relative absence of those same side effects.How I Determined Exactly How Anabolic Injectable LGD-4033 Is By Utilizing Exogenous EstradiolMost guys using injectable SARMs are using them alongside a Testosterone base at minimum.To truly evaluate the efficacy of injectable LGD-4033 in an anabolism context, all other androgens would need to be removed from the equation.As I just finished a Nandrolone monotherapy experiment prior to starting LGD-4033, my endogenous androgen production was completely shutdown.Estrogen is what has shown to be neuroprotective and not Testosterone (and potentially cardioprotective as well).Estrogen also supports several other functions in the body that would be inhibited if I were to forgo Estrogen replacement during this experiment.These include but are not limited to muscle growth and fat loss.I needed to isolate LGD-4033 and keep myself shut down to accurately assess how anabolic it is, so adding an exogenous aromatizing compound was not an option.The most common solution to insufficient Estrogen would be a Testosterone base, DHEA, HCG, or an aromatizing anabolic steroid like Dianabol or Trestolone to act as a makeshift “Test base”.None of these were viable options as they would add anabolic and androgenic activity to my body and skew my findings.The only option was to utilize exogenous Estradiol at a physiologic dose.This is because exogenous Estradiol would prevent my natural Testosterone production from turning back on (endogenous Testosterone production would also skew my findings), it would activate Estrogen receptors sufficiently to bandaid the issue of insufficient aromatization to fulfill physiologic functions, and it would not elevate androgenic activity in the body at all.In theory, by maintaining a physiologic level of Estrogen in the body I could largely avert the inhibition of anabolic pathways and assess exactly how anabolic LGD-4033 is with no factors interfering.The only potential drawback here is that aromatase is what normally regulates Estrogen production endogenously, and by bypassing this process entirely I could very well be missing out on some downstream anabolic pathways that would otherwise be fulfilled by Testosterone aromatizing into Estrogen.Just one of these being the IGF-1 pathway.The experiment is not perfect, but it is the closest I am going to get to it.Prior to my Nandrolone experiment I was maintaining my physique on 100 mg of Testosterone per week, and I was able to retain the same level of muscle mass and strength during my Nandrolone experiment with no other factors changed.If injectable LGD-4033 proved capable of maintaining my physique with no factors changed in my diet or training, then I would know that it is at least as anabolic as Testosterone and Nandrolone, but with a fraction of the androgenic activity.Oral SARMs Vs. Injectable SARMsOral SARMs have shown to have a handful of common side effects in a clinical setting, with numerous other side effects cropping up when utilized in a performance enhancing context at higher dosages.The main side effects that are consistently seen both clinically as well as anecdotally with oral SARMs are:Negative Effect On Lipid ProfileNatural Testosterone SuppressionLiver Toxicity (less common)[embedded content]Other less common side effects start to crop up once the dosage used greatly exceeds what has been evaluated on humans clinically.The potential benefits that injectable SARMs have over oral SARMs mainly come down to increased bioavailability and skipping the first pass effect in the body after administration.BioavailabilityMany SARMs have undisclosed oral bioavailability and are presumed to be low based on the lack of published data.Obviously this isn’t a scientific way to go about determining a SARM’s oral bioavailability, but until these pharmaceutical companies start to release more transparent data, researchers will speculate and make assumptions that could be true, or could be way off.Some SARMs have shown to have reasonable levels of oral bioavailability, but we don’t have exact figures for the majority of them.The closer a SARM is to 100% the closer it is to complete absorption after oral dosing.With injection, complete bioavailability is guaranteed as we are basically forcing the body to assimilate it into the blood and carry it to target tissues, whereas with oral administration we are giving the body’s oral drug metabolism an opportunity to break down the compound however it sees fit.By ensuring complete bioavailability with injection, we may be able to minimize the dosage required to yield a desired effect.In theory, this should result in less side effects and more anabolic activity milligram for milligram.This is the first potential benefit of injectable SARMs over oral SARMs.In some cases, like with SR9009 (not a SARM but is commonly lumped into the “SARMs” category), the body nearly completely breaks it down when it is administered orally, rendering it ineffective.Some oral SARMs are very bioavailable as is and we do have the data to reinforce that.For example, the SARM S23 is 96% orally bioavailable [R].This means that S23 can be administered orally, as opposed to requiring injections to achieve maximal blood serum concentration levels, which is obviously advantageous when it comes to ease of use and adoption.The First Pass Effect – Drug MetabolismDespite having nearly 100% bioavailability, oral S23 administration may have a completely different effect in the body simply by injecting it.The same could apply for any other SARM too, not just S23.After a drug is swallowed, the digestive system absorbs it and it enters the hepatic portal system.Afterwards, the portal vein carries it into the liver for metabolization, which then essentially regulates how much is filtered out prior to delivery to the circulatory system for delivery to target tissues.Not only can this process greatly reduce how much of a drug actually gets through for utilization, but it can produce a variety of side effects that wouldn’t occur with methods of administration that skip the first pass.Methods of administration like transdermal delivery or injection skip the first pass and can avoid the hepatotoxicity often associated with oral drug metabolism, as well as other side effects that can stem from the drug metabolism process itself.More often than not, this is a good thing.However, in the case of anabolic agents, it seems that the first pass can actually be responsbile for the potentiation of certain compounds, rather than the other way around.You can see how this can start to make injectable SARMs vs. oral SARMs murky territory, as we basically need to experiment with it ourselves to see if the increased bioavailability and skipping the first pass improves the anabolic activity relative to the side effect profile of SARMs, or makes it worse.For what it is worth, as of now the results seem promising, with the majority of individuals noting only drastically increased levels of anabolic activity at lower dosages, and less side effects.However, regardless of how promising and exciting this may seem, we need to consider the possibility of negative outcomes and not let the hype around injectable SARMs shroud our judgment.Examples Of How The First Pass Effect Can Greatly Impact Drug EffectsThe following are two examples of how drastic of a difference just changing the method of administration can have when it comes to a drug’s effects on the body.The first shows how injectable and transdermal estradiol was superior to oral estradiol, and the second shows how oral Superdrol was superior to injectable Superdrol (in a tissue selectivity context, not a hepatotoxicity or lipid dysfunction context).Oral Estrogen Vs. Transdermal Or Injectable EstrogenA few of the most notable drawbacks of oral estrogen pills are that they can be somewhat liver toxic, they significantly spike SHBG levels, and they result in the production of clotting factors in the blood that do not develop with forms of administration that skip the first pass.Also, the ratio of Estrone-to-Estradiol is skewed with massive elevations in Estrone with oral Estrogen administration.None of these issues occur with transdermal topical application, or injection.High levels of serum Estrone sulfate (E1S) were found after long-term oral estrogen treatment of commonly prescribed dosages, whereas there was a small increase in E1S levels after transdermal Estradiol (E2) therapy.The mean maximum E1S levels were more than 20-fold higher with oral estradiol (E2) when compared with the 0.05 mg/day transdermal estradiol patch.This is consistent with the 20-fold higher dose of E2 when compared with the transdermal dose [R].Oral estrogen also has very low bioavailability, thus requiring a much higher dosage to achieve the same effect that could be achieved with a much lower dosage of injectable estrogen.Oral Superdrol Vs. Injectable SuperdrolNot only is the side effect profile of oral Superdrol compared to injectable Superdrol substantially different, but even its anabolic to androgenic ratio changes based on the method of administration.When administered orally, Superdrol was more anabolic than methyltestosterone and several times less androgenic than methyltestosterone.Methyltestosterone has an anabolic to androgenic ratio similar to that of testosterone (close to 1:1).When administered via injection, Superdrol was nearly twice as anabolic as testosterone and twice as androgenic as testosterone.The results of subsequent assays to determine Superdrol’s anabolic and androgenic activity found that that Superdrol possessed the oral bioavailability of methyltestosterone while being 400% as anabolic and 20% as androgenic, yielding an anabolic to androgenic ratio of 20:1 [R].In the case of Superdrol, injecting it actually made it less tissue selective, despite oral administration having the obvious drawback of lower bioavailability and hepatotoxicity.My Daily Injectable LGD-4033 And Estradiol DosageAs the goal of this experiment was to determine the lowest effective dose of LGD-4033 that could replicate the same anabolic activity as 100 mg of Testosterone per week and 100 mg of Nandrolone per week, my dose was much lower than what most are utilizing in their own experiments.Once I could determine the lowest effective dosage, I could evaluate the side effect profile of that dosage, how my blood work looks on that dose, how I feel, and then make an informed decision about the overall efficacy profile of injectable LGD-4033 based on all of those factors.As injectable LGD-4033 is more bioavailable, the dosage required to replicate the anabolic activity I was shooting for would likely be much lower than you would expect via oral dosing.I spoke to Tony and Trevor about this experiment and asked for their feedback on what dose they think I should start at.They were the two who brought injectable SARMs to my attention in the first place, and nobody else I know had any experience with them at the time.At 7:02 in the following video Tony and Trevor are referring to me, and that is partially what influenced my decision to go with 3 mg per day as my daily dose.[embedded content]I also applied 2.5 grams of transdermal Estrogel (delivering 1.5 mg Estradiol) per day for the first couple weeks.I got my blood test results back from my Nandrolone experiment a couple weeks into my LGD-4033 experiment which showed that I was absorbing Estrogel very poorly, which prompted me to switch to oral Estradiol pills.My dose was 1 mg per day of Estrofem (oral 17ß-oestradiol).Ideally I would have switched to Estradiol injections, but I did not have any injectable Estradiol on hand, so I was forced to use oral pills if I wanted to maintain an optimal Estradiol level throughout the experiment.Injectable LGD-4033 Half-Life And Dosing ScheduleOrally, LGD-4033 displayed a prolonged elimination half-life (24–36 hours), linear pharmacokinetics, and predictable accumulation with multiple dosing [R].LGD-4033 dose proportional increase in systemic exposure on days 1 and 21.There was a dose-proportional increase in LGD-4033 concentrations on days 1 and 21 because of its long half-life.Serum LGD-4033 concentrations were nearly threefold higher on day 21 than on day 1, reflecting accumulation upon multiple dosing.There is not any human data we can refer to that evaluates the pharmacokinetics of injectable LGD-4033, so any statements made about how often it should be dosed are largely based on speculation and educated guesses.Tony and Trevor believe that injectable LGD-4033 can be dosed every other day and still maintain stable blood serum concentrations.[embedded content]For the sake of ensuring stability once dose saturation was reached, I maintained a daily dosing schedule from day 1 where I administered 3 mg every 24 hours.Muscle Growth And Strength Levels[embedded content]How I assess if something is working or not is by comparing it to my previous baseline metrics I have established on a therapeutic dose of TRT.If I suddenly start getting stronger while using the exact same diet and training regimen with the only factor changed being a drug, I can logically conclude that the drug is stronger milligram for milligram than my baseline on TRT.By now, I know exactly how my body responds to 100 mg of Testosterone per week, as well as 100 mg of Nandrolone per week.After swapping to injectable LGD-4033 with no other factors changed, it was very easy to assess if there were any positive or negative changes in my body composition or strength.Other than feeling a bit deflated, I didn’t experience any changes in my strength or size.My weight stayed exactly the same, my strength stayed exactly the same, and my body composition stayed the same, with the exception of being a bit flatter.Perhaps the reason I’m flatter is that LGD-4033 has less “off target” activation than something like Testosterone and Nandrolone, whereby they can increase intramuscular fullness via indirect mechanisms.That is just speculation though.At the end of the day, I haven’t lost any contractile tissue, which is the most important thing to note.I believe that a relatively low dose of injectable LGD-4033 is at least as anabolic as 100 mg of Testosterone per week or 100 mg of Nandrolone per week.While this is promising for those on TRT or who use “low” dosages of anabolic steroids, the main drawback we have seen in the past with oral SARMs is that the ceiling where diminishing returns starts to set in is far lower than with anabolic steroids.Whether or not injectable LGD-4033 has that same drawback remains to be seen.Anecdotally, other users have reported that the ceiling of diminishing returns is much higher with injectable LGD-4033, but I cannot confirm or deny this myself as that is beyond the scope of my experiment (at least for now).My only hope for this experiment was that I could retain all my muscle with just a SARM, which I did.I may consider a “blast” phase in the future where I titrate the dose up and evaluate how well it can support supraphysiological muscle growth, but that will be dictated by its androgenicity in practical application.Injectable LGD-4033’s androgenicity still needs to be explored more via further experimentation, as I did have a few red flags of androgenic activity that have me a bit hesitant to utilize a higher dose.If injectable LGD-4033 is as tissue selective as the clinical data has shown, there are several doors that open up in a bodybuilding and hair loss prevention context.Side EffectsChanges In LibidoMy sex drive went up substantially after swapping Nandrolone out for LGD-4033.Many were quick to comment on my YouTube video about how exogenous Estradiol (E2) is the reason why my libido spiked.I was already on exogenous Estradiol prior to the injectable LGD-4033 for my Nandrolone-only experiment.I have been on the same dose of transdermal E2 for almost 3 months, the only thing that changed was swapping NPP out for LGD.The libido change was from the swap.No other factors were changed.After I switched from transdermal Estradiol to oral Estradiol, my libido was no different either.The change in libido occurred almost overnight after adding LGD-4033 in.Several other individuals have come forward since that video was published reporting that injectable LGD-4033 increased their libido as well.They were all using a dose at least 5-10x higher than I was, but it is still notable nonetheless.As LGD-4033 is supposed to be so tissue selective and have such a lack of androgenicity I was very surprised that my libido spiked.If anything, I was expecting my libido to drop.With a 500:1 anabolic to androgenic ratio, obviously you wouldn’t expect one of the biggest red flags of androgenic activity to spike.Keep in mind, 100 mg of Nandrolone per week is not nothing.Despite Nandrolone being one of the least androgenic steroids ever developed (if not the least of the mainstream anabolic steroids), 100 mg per week has shown to be a high enough dose to cause virilization in women.Within 12 weeks, some women will experience virilization on Nandrolone even using only 100 mg every 2 weeks.When duration of use exceeds a year, significant virilization in women is found even at a dosage of only 50 mg every 2 weeks.My libido doubled after switching from NPP to injectable LGD-4033, which is a red flag and should be noted.My libido isn’t as high as it is on 100 mg per week of Testosterone, but it is significantly higher than on Nandrolone.Hair LossI noticed an increase in shedding using injectable LGD-4033.Further experimentation will be needed before I have a concrete conclusion on the androgenicity of injectable LGD-4033.If it ends up being hair safe, there are several applications I have in mind for this compound.Not only would it be a potent androgen receptor agonist for use in a bodybuilding context, but it could also be utilized during a hair recovery phase.For example, if you have any androgenic alopecia, periodically switching to SARMs with exogenous Estradiol (or an Estrogen precursor) in cycles could be a way to maintain muscle built via supraphysiological steroid use in the past, while reducing the androgen load on the scalp significantly enough to allow for regrowth.Or, if you don’t use steroids, it could serve as a means of recovering hair lost via endogenous androgen induced miniaturization by reducing androgenicity below baseline periodically throughout the year.Basically like a makeshift anti-androgen that won’t strip the muscle off your body.These are hypothetical examples, but these are just a few of the potential applications I see for SARMs in the future.*Update February 26th, 2020*I do not believe injectable LGD-4033 at the dosage I used is hair safe, and it may be even worse than some traditional AAS (see my blood work results video below for more elaborate details).Changes In Body Hair GrowthThis one was a metric I should have kept a closer eye on, but I usually manscape every single week so it wasn’t something I originally planned on evaluating.A few weeks into my LGD-4033 experiment I noticed that my body hair seemed to be growing a bit faster than usual.Whether this was in my head or not, I’m not positive as I was not even planning on using this as a metric, but I got backlogged on work throughout the holidays and ended up skipping my weekly manscaping sessions.While it may not be fair to say for certain that LGD-4033 increased my rate of body hair growth, I can confidently say that at the absolute least, it did not reduce my body hair growth.This is notable as well because I had no androgens in my body.If I only had Estrogen in my system and no androgens I would notice a drastic reduction in body hair growth and libido, just like transgenders who transition from male to female.The only anabolic compound in my body throughout this entire experiment was injectable LGD-4033, and I didn’t notice a reduction in androgenic activity via body hair growth either.When I crushed my DHT levels to 0 with Dutasteride, I noticed a significant reduction in back hair growth.On injectable LGD-4033, I did not notice a reduction in body hair growth at all.However, on Nandrolone I did not experience a significant reduction in body hair growth either, despite it dramatically reducing my libido.While this metric isn’t a scientific way to assess androgenic activity, in general, the body can tell you pretty accurately when androgenic activity is high or low when sufficient Estrogen is present to support erections.Increase the androgenic activity in your body and you will likely experience an increase in libido, an increase in scalp hair loss, and an increase in body hair growth (in general).Decrease the androgenic activity in your body and you will likely experience a decrease in libido, a decrease in scalp hair loss, and a decrease in body hair growth (in general).Changes In Blood PressureMy blood pressure on injectable LGD-4033 is identical to what it is normally on TRT.My blood pressure on injectable LGD-4033 and TRT is far better than it is on Nandrolone.For whatever reason, Nandrolone has a unique negative impact on systolic blood pressure, making it difficult to maintain healthy levels.On only 100 mg of NPP per week my systolic blood pressure was consistently 125-128 eating the exact same diet I was on TRT and LGD-4033.So far so good in regards to blood pressure on injectable LGD-4033 though.Changes In Resting Heart RateMy resting heart rate did not increase on injectable LGD-4033 and is no different than what it is on TRT.Potential In Preventing Or Reversing Cardiovascular Issues Caused By Steroid UseEven if injectable LGD-4033 does not end up being as purely anabolic as we hoped, there is another very promising application I see for injectable SARMs that is largely overlooked.That is the potential lack of heart stimulation.Anecdotally, many users have reported far better outcomes using SARMs than anabolic steroids in a cardiovascular health context.One example is a friend of mine, Alek Mitrevski.He used 100 mg of oral S4 (Andarine) with 0.5 mg oral Estradiol per day for over a year straight.During that time he did not experience any cardiac hypertrophy, LVH, or any kind of deleterious effect on his cardiovascular system.At the start of 2019 Alek ran a high dose Deca only cycle with Anadrol intermittently added in.[embedded content]Within 9 months, he experienced significant thickening and enlargement of his heart.He switched back to SARMs only to try and reverse this damage while maintaining the muscle he built with the Deca + Anadrol blast.Although the reports are obscure and not well documented, I have seen a handful of individuals report the reversal of cardiomyopathy and LVH after switching to SARMs only.SARMs are supposed to be tissue selective, whereas anabolic steroids have shown to significantly impair cardiac health.The potential applications this may have for athletes seeking supraphysiological muscle growth with a minimization of cardiac hypertrophy, LVH, etc. makes injectable SARMs worth further exploration in itself.Athletes seeking to reverse cardiovascular issues as a result of past AAS abuse while maintaining most (or all) of their hard earned muscle mass would also be strong candidates for benefiting from injectable SARMs if the hype around them turns out to be justified.My Blood Test Results*Update February 26th, 2020* I got my blood test results and I am adding them to the article now here:[embedded content]My commentary is also available in the video, but to put it simply, the blood test results were disappointing and I will be ending the experiment now.Reviews From Other UsersI have curated all of the injectable LGD-4033 reviews I could find and included them here for your reference as well.[embedded content][embedded content]The following comments weren’t reviews about injectable LGD-4033 specifically, but they were relevant to include nonetheless:ConclusionSome of the classic signs of androgenic activity are red flags worth keeping an eye on.But other than that, so far so good.I feel good, I am not depressed and have not experienced any negative mental or physical side effects so far despite the near complete absence of Testosterone and DHT in my body.The fact that injectable LGD-4033 has proved capable of maintaining the same amount of muscle and strength that I could maintain on 100 mg of Testosterone per week and 100 mg of Nandrolone per week is a good sign.I was hoping for that outcome, and expecting more than that is wishful thinking.If a relatively low dose of injectable SARMs can replicate the same anabolic activity of traditionally used steroids, then it is absolutely worth further experimentation.I’m going to continue digging into injectable SARMs, and I look forward to seeing more data come from other researchers in the community as well.This is a very promising area of research, and I hope that more individuals start to come forward with their personal findings too.I’ll keep you guys updated, but that is where we’re at with my injectable SARMs experiment so far.*Update February 26th 2020*My blood test results came back, and I have some concluding thoughts on this experiment I highly recommend you listen to thoroughly prior to any experimentation of your own.[embedded content]Where To Buy Injectable SARMsI strongly advise that before you buy SARMs from a company online you thoroughly evaluate their track record, their third party test results, and how they are marketing their products in general.Disclaimer: The information included in this article is intended for entertainment and informational purposes only. It is not intended nor implied to be a substitute for professional medical advice. Prior to buying anything, check that it is compliant where you live with your current government laws.Related

2020 Mr. Olympia Open Division Invites Flex Lewis To Compete
Flex Lewis Accepts Special Invitation To Compete In 2020 Mr. Olympia Open Division Flex Lewis Agrees To Compete At 2020 Mr. Olympia by Derek Hall February 6, 2020 in 2020 Mr. Olympia, Bodybuilding, Mr. Olympia, News Fans have been wondering whether or not we would see Flex Lewis compete at the 2020 Mr. Olympia. That wait is over, as it has…
Does The Fittest Man On Earth Really Consume 9,300 Calories A Day!
Does The Fittest Man On Earth Really Consume 9,300 Calories A Day! Crossfits Mat Fraser Shares His Daily Diet and Nutrition Habits by Derek Hall February 4, 2020 Photos via Instagram @mathewfras It comes as no surprise that someone as active and athletic as Mat Fraser needs to eat a ton of calories. However, you would not…
Dumbbell Bench Press Guide: Benefits, Performance, and Variations
If you’ve ever had a chat with a fellow gym-goer about your workouts, invariably, the discussion will turn to the bench press. Why? Because it’s probably the most popular upper body exercise on the planet. Even non-lifters want to know how much you can bench press! Most of the time, people are talking about the…

Clenbuterol cycled with IGF-1 lr3 to Lose Fat While Adding Lean Muscle
Clenbuterol cycled with IGF-1 lr3 to Lose Fat While Adding Lean Muscle Please visit the MuscleChemistry Peptide and HGH Forum To Learn More, Ask Questions, and Read Reviews on everything from your basic PCT ancillaries, to HGH, IGF-1 lr3 and Much Much More! 1. IGF-1 lr3 Stacked with Clenbuterol By far the best way…
Deca Only For HRT – A Comprehensive Overview And My Personal Blood Work
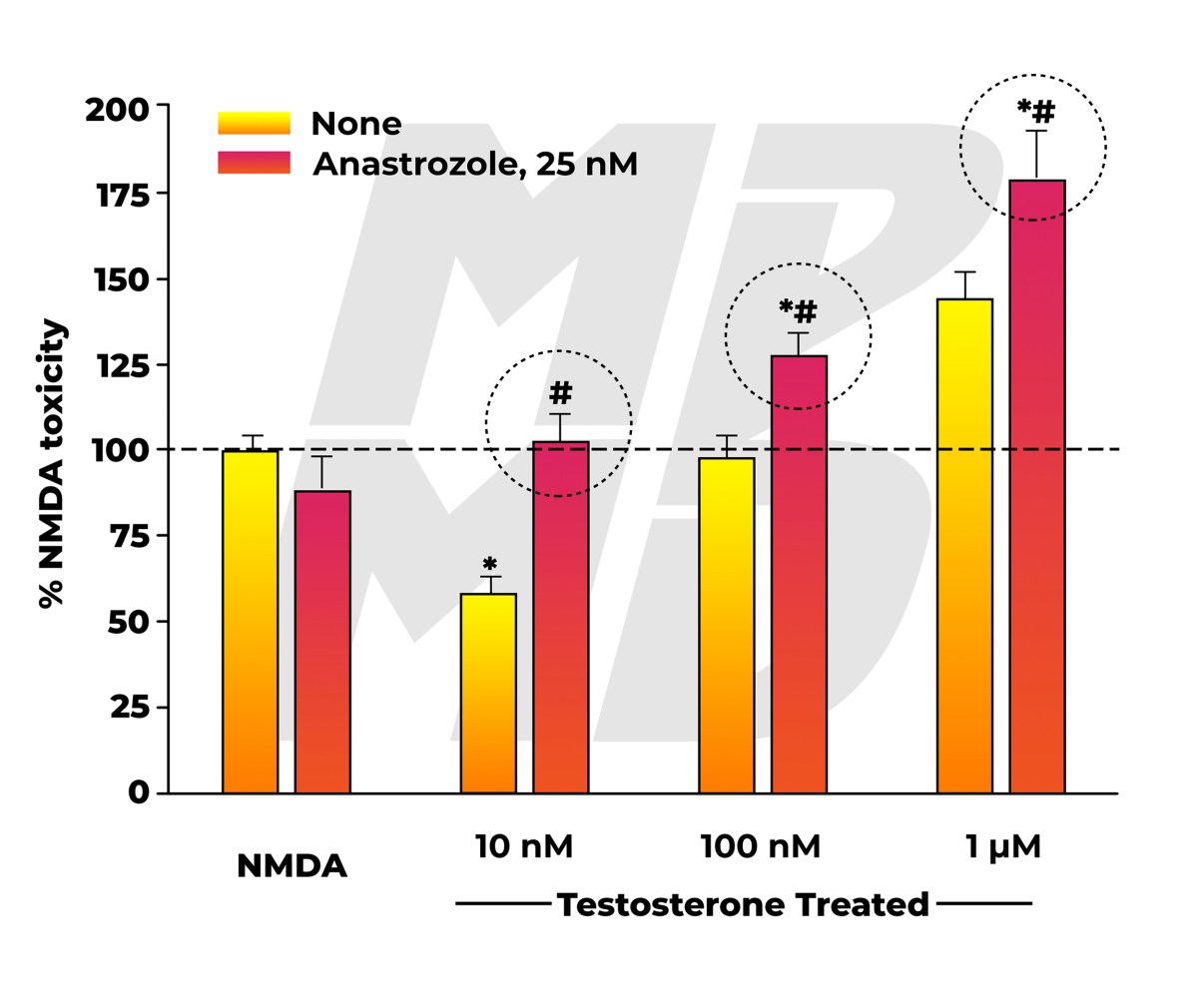
There’s been a growing amount of hype around the “Deca only cycle”.While it is most commonly referred to as the Deca only cycle, it is actually based on the compound Nandrolone being used on its own.The decanoate ester being abbreviated as “Deca” has just become synonymous nowadays in the bodybuilding community with Nandrolone itself.Seeing the potential merits of Nandrolone as a makeshift hormone replacement therapy alternative to Testosterone, I stopped using Testosterone and instead started using Nandrolone on its own with exogenous Estradiol for 3 months and paid over $1000 for an elaborate blood panel to assess how it affected my health markers.[embedded content]Table of ContentsHow Nandrolone Could Potentially Be A Superior HRT Alternative To TestosteroneThe primitive thought process is that Nandrolone used in conjunction with Testosterone will lead to horrible side effects, but Nandrolone used on its own will just result in all of the benefits of steroids with a near absence of the androgenic or estrogenic side effects associated with Testosterone use.In reality, it’s a lot more nuanced than that.The reason why I found this experiment worth pursuing is the lack of androgenicity of Nandrolone in the body.Nandrolone 5α-reduces in tissues that express 5α-reductase to the much less androgenic metabolite Dihydronandrolone (DHN).Nandrolone is basically the only anabolic steroid that is going to maintain 100% anabolic activity of the Nandrolone in muscle tissue where you want it, but also be converted into a much less androgenic metabolite with a lower binding affinity in certain areas of the body where you wouldn’t want Nandrolone to bind.The two areas of concern for most individuals being hair follicles and skin.By converting to DHN in these areas, Nandrolone (and by extension DHN) causes less hair loss and acne than Testosterone (and by extension DHT).In addition, some men are genetically predisposed to high levels of aromatization and estrogen receptor expression and can’t even use TRT doses of Testosterone without experiencing estrogenic side effects.Nandrolone is not a potent substrate for aromatase, and mainly converts to a weaker estrogen called Estrone (Estradiol is about 10-fold more potent than Estrone).Nandrolone is also mildly estrogenic on its own via its ability to act as an estrogen receptor alpha (ERα) agonist [R].Overall, Nandrolone is much less androgenic and estrogenic than Testosterone, and may provide symptom relief in those seeking a viable hormone replacement therapy alternative.In this context, Nandrolone may also have great potential as an efficacious alternative to Testosterone as an anabolic agent for some individuals who are prone to androgenic and/or estrogenic side effects.The Neurotoxicity And Cardiotoxicity Of NandroloneBased on the limited data available, Nandrolone has shown to be more deleterious to cardiovascular and neurological health than testosterone.[embedded content]By extrapolating the data, we start to get a clearer picture as to why this likely is.Nandrolone is mildly estrogenic on its own, and it does not aromatize nearly enough to create as much Estradiol as Testosterone does.Comparing the effect of testosterone with that of 19-nortestosterone (Nandrolone) and Stanozolol (Winstrol) on neurotoxicity we can clearly see that Estrogen is what protects neurons in the brain, not Testosterone itself.In this study, a physiologic dosage of Testosterone was neuroprotective [R].Testosterone only amplified neurotoxicity at supraphysiological dosages.The neuroprotective effect of a physiologic dosage of Testosterone was completely eliminated when the aromatase inhibitor Anastrozole (Arimidex) was co-administered, suggesting that the intrinsic toxicity of Testosterone as an androgen is only counterbalanced by its aromatization into 17β-estradiol.As opposed to testosterone, Nandrolone does not appear to aromatize sufficiently into estrogen.As you would expect, Nandrolone was neurotoxic at every single dose evaluated regardless of Arimidex being co-administered or not.If Nandrolone was inherently able to provide enough estrogen receptor alpha (ERα) activation to balance out its androgenicity without even requiring aromatization (it acts as an estrogen on its own to some extent), we would see a neuroprotective effect at equivalent dosages to a physiologic concentration of Testosterone when no AI is used, but that does not appear to be the case either.The anti-androgen flutamide attenuated the neurotoxicity of all three androgens, thus further reinforcing that physiologic dosages of androgens without a sufficient amount of opposing estrogens, or supraphysiological dosages of androgens may facilitate neuronal death.I suspect that the same applies for the inherent cardiotoxicity of Nandrolone as well.Just because you can get your Estradiol levels up to 15 pg/mL with a gram of Deca only, that ratio of androgens to estrogen in the body is way off of what would otherwise be optimal for health based on what I’ve seen.This is reinforced by the fact that Flutamide (an anti-androgen) was able to attenuate the neurotoxicity of Nandrolone.By preventing Nandrolone from binding to androgen receptors, it is no longer able to transcribe its effects in tissues.Hair loss and acne are one thing, cardiotoxicity and neurotoxicity are another thing and should ultimately take precedence obviously.However, just because Nandrolone monotherapy cannot produce a sufficient ratio of androgens to estrogens, that doesn’t mean that there isn’t a potential loophole.That loophole is exogenous Estradiol administration.Exogenous Estradiol Use With Nandrolone Only CyclesAs we’ve seen, Estrogen produced via aromatase is what provides neuroprotection from the androgenicity of Testosterone, not the Testosterone itself.We also know that Nandrolone is not able to produce enough estrogenic activity in the body to facilitate this same level of neuroprotection.I theorize that Nandrolone in conjunction with exogenous Estradiol to replace this otherwise missing component could attenuate a significant amount of the deleterious impact Nandrolone has on the heart and brain.In addition, by providing a sufficient amount of exogenous estrogen, libido, muscle growth, fat loss, and several other aspects of health and performance should be more optimized.It isn’t a coincidence that cardiovascular disease rates skyrocket once women hit menopause and stop producing Estrogen properly.The same negative effects will apply in men with low Estrogen levels.The lack of sufficient Estrogen is often addressed in Deca only cycles by adding an adjunct anabolic steroid that aromatizes into Estrogen or Estrogen analogs.Obviously for those seeking to minimize androgenic side effects, the ideal way to go about achieving sufficient Estrogen receptor activation is probably not going to be by adding more steroids to their protocol.This is where exogenous Estradiol comes into play, and I believe the majority of Deca only cycles would be more sustainable from a health perspective, and successful in a bodybuilding context as well with its inclusion.I have yet to see one person on a Deca only cycle achieve a sufficient Estradiol level relative to their Nandrolone dosage via a sensitive assay Estradiol blood test.The following blood test result was submitted by an individual on over 1000 mg per week of Deca only.Over a gram of androgens relative to a 19.2 pg/mL Estradiol level is far from ideal in my opinion.I had a good conversation with Vigorous Steve as well about his Deca only cycle experience.He told me that his Estradiol was 12 pg/mL on 1000 mg of Deca per week after 4 weeks, and he ended up adding 25 mg DHEA per day just to bring it up to 25 pg/mL.When it comes to Nandrolone use on its own, most would benefit from more Estrogen in my opinion.My Weekly Nandrolone And Estradiol Dosage For “HRT”Most guys doing Deca only cycles are evaluating Nandrolone at dosages of 600 mg or higher per week for short blasts.My experiment was based on its potential as an alternative long term HRT option for those prone to androgenic side effects.Or alternatively, its potential as a compound to swap to periodically throughout the year from TRT to reverse some of the androgenic side effects of Testosterone and DHT while still maintaining the same amount of muscle mass.Every blood test I’ve seen of Deca only cycle users was on high doses of Nandrolone without a sufficient amount of Estrogen.I wanted to see how Nandrolone on its own at a “therapeutic dose” would affect my blood work if I had a sufficient amount of Estrogen provided through exogenous Estradiol.Long-term, the only way Nandrolone monotherapy could be even relatively safe in a cardiovascular context would be with exogenous Estradiol supplementation from what I’ve seen.And even then, I’m sure it has major drawbacks that will likely accumulate over the years.With that being said, it is still something I wanted to explore nonetheless, as it is one of the few compounds that can actually support supraphysiological muscle growth with a relatively minimal impact on androgenic alopecia.Oral micronized Estradiol tablets have quite a few drawbacks.A few of the most notable drawbacks are that oral Estrogen pills can be somewhat liver toxic, they spike SHBG through the roof, and they result in the production of clotting factors in the blood that do not develop with forms of administration that skip the first pass.The two most viable methods of administration that skip the first pass are transdermal topical application, or injection.I chose to topically apply transdermal Estradiol gel (Estrogel) for this experiment.I used 100 mg of Nandrolone phenylpropionate (NPP) per week split into daily injections using an insulin pin rotating between my glutes and ventroglutes.I also applied 2.5 grams of transdermal Estrogel (delivering 1.5 mg Estradiol) to my inner thighs every day for over 3 months straight.Blood Pressure Changes On NandroloneOne of the first things I noticed was that it was a struggle to keep my blood pressure in check on NPP, even at the mild dose I was using.What that was caused by exactly, I’m not sure.I assumed it was Aldosterone prior to this blood work.When I’m on Testosterone, even when I was using TRT as high as 200 mg per week, I could keep my blood pressure at 110/70 with ease.Even if I ate terribly, I could still hold 115/75 without even trying on Testosterone.Within the first week of switching to NPP it became way harder to control my systolic blood pressure.My diastolic blood pressure was fine for the entire 3 months, but my systolic blood pressure would consistently be around 125-128.That is not normal for me, and is borderline stage 1 hypertension.The fact that I even had to try to lower my blood pressure showed to me that Nandrolone is a lot harder to manage in this regard.This is consistent with almost every single person I know who has blasted high doses of Deca.They all had significant issues with blood pressure.Most of the guys who thought they had normal blood pressure were actually stage 1 hypertensive and didn’t even realize that their results were indicative of cardiovascular stress.My 125-128 systolic occurred without being in a calorie surplus, without any weight changes, and on what I would consider a very low dose of NPP.The exact same diet, weight, lifestyle, etc. would have me at 110/70 on TRT.Muscle Growth And Strength On NandroloneI maintained my muscle and do not feel that there was a substantial difference between the anabolic potency of Nandrolone compared to Testosterone.At the very least, the anabolic activity of Nandrolone is comparable to Testosterone, but the androgenic activity is far less than that of Testosterone.In certain contexts for certain individuals, Nandrolone will be the desirable alternative because of this.Reduced Libido On Nandrolone – Deca Dick?My libido was extremely subdued on NPP.That’s one of the most obvious things I noticed during my experiment.I had a libido and would still want to have sex, but my libido was much lower than it is on regular TRT.On TRT I can barely go one day without sex before it starts to consume my mind. On Nandrolone only, I can easily go a couple days barely even thinking about it.However, when it came time to get the job done, I could still get the job done and stay hard the entire time without any issues in erection quality.It was a bit harder to reach orgasm though.On top of the lack of androgenicity causing a reduction in libido, Nandrolone also has progestogenic activity and binds to the Progesterone receptor.Excessive Progesterone is notorious for killing libido and causing erectile dysfunction, and it seems that Nandrolone has similar effects in many individuals via this pathway in conjunction with its 5α-reduction into DHN.My drive was also lower, and I felt less aggressive overall.In many individuals Testosterone and DHT levels will strongly influence libido, drive, aggression, motivation and productivity.Personally, even if I have that support via DHT or DHT derivatives, the increased motivation and drive is actually more counterproductive in a work productivity context because my libido gets way too high.Even when I had high testosterone levels and 0 DHT in my body I still had sex on my mind far more than I would like.When that happens, I can barely get anything done, and then I end up depleting myself of energy for the day through excessive sex.The subdued and normalized libido on Nandrolone is welcomed for me because of this.I don’t think this is necessarily just because I’m a good responder to Nandrolone, I think it has more so to do with the fact that I was using exogenous Estrogen during this experiment with the Nandrolone.Despite androgens driving aggression and drive, libido and erection quality is largely dictated by adequate Estrogen levels.With all that being said, DHT (with sufficient Estrogen via Testosterone aromatization) is blatantly better for sexual support than Nandrolone, and testosterone itself, even if you completely inhibited 5α-reductase and nuked DHT, still provides better libido and erection quality than Nandrolone does at equivalent “therapeutic” doses for the majority of people.My Blood Work Results On A Deca Only Cycle For HRTI don’t like taking shots in the dark when it comes to something that I see potential in.There is a lot of theory thrown back and forth in the community on Deca only cycles, and I needed to see for myself how Nandrolone in conjunction with exogenous Estradiol would impact my personal blood work.I wanted to check markers of oxidative stress, inflammation, kidney function, Aldosterone, Prolactin, hormone levels via sensitive assay testing, and an array of other health markers that are often debated about but very infrequently actually tested for to reinforce statements made.Expectedly, high dose Deca only cycle blasts will almost always result in low HDL levels, subpar Estradiol levels, and an array of other out of range values that are less common and are more individual dependent.To date I have yet to see someone get their blood work checked with exogenous Estradiol being used in conjunction with Nandrolone at a “therapeutic” dose.This is what I wanted to evaluate.Complete Blood Count with Differential/PlateletsI was actually expecting far worse from my blood test results.At a “therapeutic” dose, it doesn’t seem like my hematology was negatively affected at all.Comprehensive Metabolic PanelIn my metabolic panel, nothing was really off to the point that would cause concern.My BUN being high is likely just the result of being muscular and having a high protein diet.Lipid PanelGoing into the lipid panel, we can see the number one most common blood test result among steroid users.My HDL is low.LDL is also borderline high, but not overly concerning when I can see that my Triglycerides are pretty low.The reason why my HDL was too low was that my Estrogen levels were too low.Again, this just reinforces the fact that Nandrolone does not sufficiently aromatize into Estrogen.I will get into my Estrogen level and why it was still too low even with Estrogel administration later once we get to that part of the blood test results, but my HDL could have been in range if my Estrogen level was in check.If I didn’t use the Estrogel my HDL likely would have been in the single digits.I know I can get my HDL into the reference range if my estradiol levels were doubled, which I have the leeway to do.Iron And Total Iron Binding CapacityGetting into Iron and TIBC we can see that everything looks pretty normal here.Total Testosterone And Free TestosteroneExpectedly, by assessing my Total Testosterone level via liquid chromatography with tandem mass spectrometry (LC/MS-MS) and my Free Testosterone level via equilibrium ultrafiltration, we can see that my Testosterone levels were crashed.Both the total and the free were lower than a healthy female.This is what you should see in your blood work if you’re on just Nandrolone.The only Testosterone being produced in my body was indirectly via the trace amounts of androgens produced in my adrenal cortex, which is why the value wasn’t completely bottomed out at 0.I’ve mentioned many times the importance of getting high sensitivity testing done for hormone levels and how Nandrolone will register as Testosterone in primitive garbage blood tests.This is another great example of this.In addition to high sensitivity testing, I had the same blood tested using electrochemiluminescence immunoassay (ECLIA) for my Total Testosterone level, and direct analog enzyme immunoassay (EIA) for my Free Testosterone level.These were the test results using the exact same blood sample with the terrible default assays that doctors will use to determine how to treat you, and that labs will give you in the majority of your blood work panels.According to ECLIA and EIA, I have a normal Total Testosterone and Free Testosterone level.Hilarious.This just one example of why getting accurate hormone testing is critical.My Testosterone levels are actually in the gutter, but the stupid primitive tests that doctors and labs give out as defaults for people is so f*cking stupid that it can’t even tell the difference between Testosterone and 19-nortestosterone in my blood.Renin Activity and AldosteroneMy renin activity and Aldosterone appeared to be normal.This is one of the main things I wanted to check because there’s a lot of speculation around the effect Nandrolone is going to have on Aldosterone levels.When it comes to the Deca only cycle, there’s something going on that throws off homeostatic mechanisms that regulate blood pressure that does not appear to be Estrogen related or Aldosterone related.At least based on my blood work, my Aldosterone was definitely not at a level that could imply any kind of negative effect on blood pressure.My Aldosterone level was low if anything.Granted, some markers in the serum can be relatively worthless when compared to actual tissue concentrations, but at least based on my blood work, Aldosterone does not appear to be the culprit.The first thing many jump to when explaining blood pressure regulation is the effect Nandrolone supposedly has on spiking Aldosterone through the roof, but it just doesn’t appear to be the case in my experience as you can see yourself here.Vitamin B12 and FolateMy B12 and Folate levels were normal.PregnenolonePregnenolone appeared to be normal and within the reference range for men which is notable, as many assume that Nandrolone will shut down the production of precursor steroids.That does not appear to be the case either.I assumed precursor hormone levels like Pregnenolone would be less affected than many seem to think as most circulating Pregnenolone is derived from the adrenal cortex.Dihydrotestosterone (DHT)Expectedly, my DHT was very low.This is because I have almost no Testosterone being produced to 5α-reduce into DHT.If my Testosterone is low, my DHT will be low as well.DHT Backdoor PathwayContrary to popular belief, there is a backdoor pathway via Pregnenolone that can create DHT as well, which contributes to the chunk of DHT I have in my blood.Hemoglobin A1cHemoglobin A1c appeared to be normal at 5.1%.Thyroxine (T4)My Free T4 was 1.28 ng/dL, which is acceptable.DHEA-SulfateMy DHEA was in range and actually on the high end of normal.Being on exogenous Nandrolone or Testosterone does not shut down DHEA production.CortisolCortisol was “normal” apparently, although it looks a bit high to me.I believe this result was mostly sleep hygiene related rather than entirely Nandrolone related.Thyroid Stimulating Hormone (TSH)My TSH is too high.I’ve never had a TSH this high before.I have had a TSH in the 2’s before, this isn’t the first time, but never this high.However, based on my resting heart rate and my morning waking temperature and my mid-day temperature, my metabolic rate seems to be the same as it usually is on TRT, and I have had no standout hypothyroidism symptoms.Luteinizing Hormone (LH) and Follicle Stimulating Hormone (FSH)Expectedly, LH and FSH were undetectable.ProlactinMy Prolactin was on the low end of normal.This was another interesting health marker to see on Nandrolone, as many will often jump to assuming that Nandrolone spikes Prolactin levels through the roof.That does not appear to be the case though.Prostate-Apecific Antigen (PSA)My PSA level was normal, and did not change from my previous blood work on Testosterone for TRT.D-DimerMy D-Dimer was normal.A friend of mine had a very high D-Dimer level on a Deca only cycle and he wanted me to check mine to see if there was a pattern.It looks like the elevated D-Dimer was case-specific for him and was probably caused by something completely unrelated, as my D-Dimer is normal.C-Reactive ProteinC-Reactive Protein is one of the primary markers we have for assessing inflammation in the body.A C-Reactive Protein level of 0.34 mg/L is not overly concerning, although I would like to see it below 0.3 mg/L.I had undetectable C-Reactive Protein levels in the past on TRT, and on Nandrolone it jumped up to 0.34, which is notable.Estradiol, SensitiveMy Estradiol (E2) level determined via LC/MS-MS was only 15.4 pg/mL, despite administering 2.5 grams of Estrogel per day.This was disappointing, as I would have liked to see my E2 at least around 30 pg/mL based on the amount of Estrogel I was applying daily.Evidently, my inner thigh was not absorbing the Estrogel very well.This is one of the recommended areas of application, but my results were not even close to in line with the average blood levels found in the Estrogel pharmacokinetics studies.With daily administration of 2.5 g or 5 g Estrogel (corresponding to 1.5 mg or 3 mg estradiol, respectively), mean serum estradiol concentrations of approximately 80 pg/ml (294 pmol/L) and 150 pg/ml (551 pmol/L), respectively, are maintained.Administration of Estrogel also results in increased serum estrone concentrations, producing a physiological estradiol/estrone ratio of approximately one.Therefore, serum concentrations of both estradiol and estrone and the serum estradiol/estrone ratio provided by ESTROGEL® are consistent with physiological levels observed during the follicular phase of the normal menstrual cycle.My inner thigh isn’t very hairy at all as I manscape fairly regularly, so I expected at least a 40 pg/mL E2 based on the amount of Estrogel I was applying.I was overly generous with my dose based on the off chance that I would encounter an absorption issue, and my E2 was still way below where I expected it to be.Based on the pharmacokinetics outlined by Merck, 80 pg/mL is the average E2 level for someone applying 2.5 grams of Estrogel per day.There’s no way I could have predicted that I would have an absorption issue so problematic that it would result in five times lower absorption than the average.If my E2 was closer to 30 pg/mL, I expect that my HDL would have been pushed into the reference range, and all Estradiol driven physiologic functions likely would have been more optimized.To me, this just reinforced further that Nandrolone is a subpar source of Estradiol as I was using a high dose of transdermal E2 and still could barely reach a satisfactory E2 level.To increase my E2 levels for similar future experiments I will either have to find a better application area, add some DMSO to my Estrogel to increase absorption, or consider Estradiol injections instead.HomocysteineMy Homocysteine level was higher than I would like.Normally my Homocysteine is closer to 8-8.5 umol/L.Earlier in the year when I did a shorter Nandrolone experiment for a month using 200 mg per week (double the dose I used for this experiment) I had a Homocysteine level around 8.5, so I doubt this spike was Nandrolone related.This is one of the main markers I always have my eye on because I am homozygous for the C667T polymorphism.Gamma-Glutamyl Transferase (GGT)My GGT looked good.I was worried that this would be cranked through the roof as it is a marker of oxidative stress.MagnesiumMy magnesium level looked okay.Copper and ZincMy zinc level looked okay.My copper level may be a bit low, which I am now addressing by eating an ounce of beef liver every day.ProgesteroneMy Progesterone was normal, which is notable as it is another precursor hormone that many assume drops to zero when exogenous anabolic steroids are present in the body.InsulinMy insulin level was good.EstroneExpectedly, my Estrone was a bit high.This can be a major problem with exogenous Estradiol and Nandrolone unfortunately.Estrone Level Increase From Exogenous EstradiolThe ratio of Estrone-to-Estradiol is skewed with massive elevations in Estrone with oral Estrogen administration.Fortunately, this unhealthy ratio can be avoided for the most part with transdermal Estradiol administration.High levels of serum Estrone sulfate (E1S) were found after long-term oral estrogen treatment of commonly prescribed dosages, whereas there was a small increase in E1S levels after transdermal Estradiol (E2) therapy.The mean maximum E1S levels were more than 20-fold higher with oral estradiol (E2) when compared with the 0.05 mg/day transdermal estradiol patch.This is consistent with the 20-fold higher dose of E2 when compared with the transdermal dose [R].Estrone Level Increase From NandroloneNandrolone also significantly elevates concentrations of Estrone in plasma [R].During a pilot study evaluating the possible beneficial effect of Nandrolone Decanoate (ND) on bone metabolism in patients with rheumatoid arthritis there was a significant increase in the serum levels of Estrone [R].Despite the fact that Estrone can convert to Estradiol, we can clearly see that the amount this actually happens in the body is minimal based on the consistently skewed ratios of androgens to Estradiol in the blood test results of Deca only users (or Nandrolone in general).FerritinMy Ferritin level is too low.This is likely the result of phlebotomizing too frequently in 2019.EstriolMy Estriol level was undetectable, which was expected.Triiodothyronine (T3)My Free T3 level was 2.7 pg/mL.It’s not low enough for me to be overly concerned, however, it is suboptimal and should be in the low 3’s at least.This is something I will need to address moving forward.With that being said, I like to look at my resting heart rate as well as my body temperature for a more accurate assessment of my metabolism, and both are where I want them to be.My waking temperature has consistently been 98 degrees Fahrenheit, and my midday temperature has consistently been 98.6 degrees Fahrenheit.Sex Hormone-Binding GlobulinExpectedly, my sex hormone-binding globulin (SHBG) was low.While this isn’t as relevant for a Nandrolone only user as Nandrolone has a very low affinity for SHBG, this is a value I would still like to see in the reference range, especially if I was on TRT.If I had the Estradiol level I was shooting for, I’m confident that my SHBG would have been in the reference range.My Overall Experience On Nandrolone And Exogenous Estrogen For HRTI was expecting to see a bunch of red flags in my blood work, but nothing really stood out as a major concern to me except for the spike in systolic blood pressure, and the high Estrone level.A before and after echocardiogram and calcium scoring would have been nice to see, but unfortunately I can only afford to do so much in these experiments, and the blood work was expensive enough as is.I felt good throughout the entire experiment, I maintained my physique, my libido and penis were functional, and my blood work looked pretty good considering that each issue was something more so related to my Estradiol administration than the Nandrolone itself.Estrone being out of range is a concern, as I would need to use even more exogenous Estradiol to achieve what I would consider a more therapeutic E2 level, which would likely push my Estrone up even higher.The difficulty in controlling the blood pressure spike is also a huge concern and could be a deal breaker.If I gave this experiment more time, it is entirely possible that certain things would have become problematic that appeared to be fine during my three month assessment, like my libido or sense of well-being.It is also possible that despite maintaining a healthy Estrogen level, the same neurological and cardiovascular issues we see in a significant amount of the Nandrolone data could still accumulate over time.In addition, healthy looking serum levels of Estradiol may not necessarily reflect adequate localized Estrogen receptor activation in each tissue.With Testosterone, there is a regulated amount of aromatization occurring in each tissue to satisfy however much Estrogen receptor (ER) activation we need.In the context of Deca only cycles, or Nandrolone monotherapy, there’s nothing else I can refer to other than serum levels, my libido, sense of well-being, other cardiovascular health markers, etc.In other words, just because you feel good and your Estrogen levels look good on paper, that doesn’t mean that an exogenously administered source of Estrogen is providing the same therapeutic ER activation in all tissues like it would if it were regulated via aromatase.With that being said, you could also argue the opposite as adequate receptor activation via exogenous hormone therapy is essentially all HRT boils down to to begin with in the context of any hormone.More than 95% of our endogenous Testosterone is produced in the testes.Testosterone is supplied to target tissues in the blood, just like most other hormones in the body.If you inject exogenous Testosterone, it then goes into the blood and is supplied to target tissues.If you inject anything it goes into the blood and then is carried to the areas that it is needed.Estrogen replacement has been deemed satisfactory for fulfilling the same functions as endogenously produced Estrogen in women for years, and synthetic Estrogen analogs are handed out like candy to millions of young girls (including teenagers).Is it healthy?Estrogen analogs like Ethinyl Estradiol probably aren’t ideal for regulating Estrogen dependent functions, and they definitely aren’t ideal for developing women who haven’t fully matured.However, there is tons of data to support the fact that exogenous Estradiol is well-tolerated, has a strong safety profile, and can still fulfill physiologic functions sufficiently.In an ideal world, this would be a regulated process in the body in each tissue (aromatization).My experiments do not necessarily reflect what I believe are best practice with these hormones, which should be noted.This was an experiment, and not something that I would recommend someone else do.Using an exogenous progestogen with estrogel certainly isn’t what I would consider an optimal HRT protocol, or what is indicative of an ideal means of providing androgenic and estrogenic support in tissues.With that being said, I don’t see a better way to go about utilizing Nandrolone on its own for HRT.Should it even be considered as an HRT alternative though?That’s the question, and I believe it is largely going to be individual dependent, with a significant amount of users having poor outcomes in one aspect or another.I do believe there are a minority of individuals who are very prone to androgenic and/or estrogenic side effects from exogenous Testosterone use that may benefit from exploring Nandrolone though, and it should not be discarded as a potentially viable alternative simply because it is not the primary bioidentical hormone that men produce.Related
Testosterone Is NOT Neuroprotective, Estrogen Is – Anabolic Androgenic Steroid Neurotoxicity
Testosterone is not neuroprotective, estrogen is.A common myth circulating in the bodybuilding and TRT community is that testosterone is inherently neuroprotective and is unique from all other anabolic steroids in that regard.The reason why testosterone is neuroprotective is simply because it aromatizes at a rate that provides a sufficient amount of estradiol to balance out the androgenicity in the body.Data in rodent models using cortical cells suggests this very convincingly by showing how the aromatase inhibitor Anastrozole (Arimidex) completely eliminated the neuroprotective effects of testosterone [R].[embedded content]Table of ContentsAre Synthetic Anabolic Steroids More Dangerous Than Testosterone?There have been tons of studies published suggesting how much worse synthetic anabolic steroids are in contrast to testosterone for cardiovascular disease, neurotoxicity, and a myriad of other deleterious outcomes. I believe that a significant amount of this data is exaggerated based on the fact that exogenous estrogen is never co-administered in these studies.At the end of the day, testosterone is the safest androgen at physiologic dosages. However, I theorize that many synthetic anabolic steroids are not as dangerous as we are led to believe. My theory is that some compounds are not inherently significantly more dangerous than testosterone, rather, it is their lack of aromatization, 5-alpha reduction, or differing affinity for off-target receptors that makes them more dangerous.The effect on estrogen receptors and how potent of a substrate an anabolic steroid is for aromatase is the main factor that impacts how viable a hormone is for consideration in a monotherapy context.DHT derivatives cannot be converted by the enzyme aromatase into an estrogen like estradiol.Nandrolone (19-nortestosterone) and its derivatives (19-nors) each have their own individual affinity (or lack thereof) for estrogen receptors and interaction with aromatase, often resulting in subpar estrogen levels (exceptions to this exist such as Trestolone/MENT).Basically, I believe that some steroids may show to be significantly more cardiotoxic and neurotoxic in the data because they are always used on their own with an insufficient amount of estrogen to balance out the androgenicity in the body.The Importance Of Sufficient Estrogen LevelsHealthy estrogen levels are needed for libido, erection quality, vasodilation, cardiovascular health, brain health, bone health and several other critical functions.In women the risk of cardiovascular disease spikes significantly after menopause.It isn’t a coincidence that the majority of women who develop heart disease have it occur after their estrogen production has dropped to sub-male levels.If you don’t have a sufficient amount of estrogen relative to androgen levels in the body, cardiotoxicity and neurotoxicity levels will be significantly higher than they would be if healthy estrogen levels were sustained.From a bodybuilding perspective, estrogen is needed to optimize muscle growth, fat loss, as well as IGF-1 and growth factor production/cellular signaling.This is why heavily aromatizing steroids may indirectly result in greater growth potential and are often classified as “bulking” compounds.Anecdotally, many bodybuilders report that the most they’ve ever grown was during off-season mass building phases when their estrogen levels were through the roof.The Point Of A Testosterone BaseTestosterone is not tissue selective and is actually a poor muscle builder milligram for milligram when compared to other synthetic anabolic steroids developed in the years following its discovery.When it comes to nitrogen retention, on paper it is not superior to many anabolic steroids.However, it aromatizes into estradiol at a very tightly regulated rate, it is bioidentical, and our body knows exactly what to do with it.In addition, our body knows how much testosterone to bind up with SHBG, how much to free up and make available to tissues, as well as how much DHT to 5-alpha reduce to antagonize estrogen receptor activation should it get out of control.From a bodybuilding perspective, testosterone is subpar in many aspects.However, in an overall health, longevity AND bodybuilding context, testosterone cannot be beat at therapeutic dosages.By using a testosterone base or a source of sufficient estrogen the shortcomings of other anabolic agents can be attenuated to some extent, hence why testosterone is the base of most steroid cycles.The Balancing Act Of Testosterone, DHT and EstrogenSteroidogenesis in the body is carried out like a massive orchestra to regulate countless functions.It’s far more elaborate than simply testosterone, estrogen and DHT production.Even at a snapshot view, the balancing act of androgens and estrogens in the body is tightly regulated and is carried out to ensure health remains optimized.This balancing act gets more and more dysfunctional with age, poor lifestyle, poor diet, poor sleep hygiene and numerous other factors.However, the body still knows exactly what to do with testosterone, how to create an optimal opposing amount of estrogens, and how much testosterone to 5-alpha reduce into DHT to oppose excessive estrogens and support male secondary sex characteristics.When you compare clinical data on a synthetic anabolic steroid to testosterone in a monotherapy context, you have to consider that these studies are utilizing that synthetic steroid on their own, not with exogenous estrogen or any supplementary hormones that may be needed to balance out its androgenicity, lack of estrogenic activity and/or interaction with aromatase.Obviously if you take a compound that doesn’t aromatize sufficiently to estrogen and compare it head to head with the bioidentical androgen that our body knows how to aromatize and 5-alpha reduce at a perfectly balanced rate, you can just imagine which is going to come out on top in a cardiotoxicity and neurotoxicity context.Does this mean that a synthetic anabolic steroid compared to testosterone would not potentially be more efficacious than testosterone should those other backend pathways be supplemented to fill the gaps though?Synthetic Anabolic Steroids With Exogenous Estradiol For HRTSome individuals have underlying genetic polymorphisms and defects in sex hormone metabolism that may throw off the tightly regulated steroidogenesis pathway in a way that skews too heavily in favor of estrogen, or too heavily in favor of androgens.There are many cases in which synthetic anabolic steroids may beat out testosterone, despite testosterone on paper being the candidate of choice for most men at therapeutic dosages, and still the candidate of choice for many men at supraphysiological dosages too in a bodybuilding context.Nandrolone is a great compound to exemplify this in my opinion.It has a much lower level of androgenicity in the body due to its 5-alpha reduction into DHN, and it is also far less estrogenic than testosterone.Those who are prone to gyno, hair loss, acne or other common testosterone related side effects typically prefer nandrolone for this reason.This is why many female oral contraceptives are nandrolone analogs as well.Unfortunately, your heart and brain don’t care if you have hair loss, acne, or gyno, so there can be deleterious outcomes as a result of androgen use without a sufficient amount of unopposed estrogens, or an estrogen excess without sufficient androgen opposition.In regards to nandrolone, I don’t believe it has a sufficient amount of opposing estrogen to balance out its androgenicity.It activates estrogen receptor alpha (ERα) a bit via its inherent estrogenicity and it can aromatize to estrone, which can then convert to estradiol, but the amount of overall estrogenic activity it provides does not appear to be sufficient to offset its neurotoxicity or cardiotoxicity.I believe this is why most of the data found in nandrolone studies shows how horrible it is for the brain and the heart.Nandrolone is always evaluated on its own without a sufficient amount of estrogen present to provide cardiovascular and neurological support.If you shut down your natural endogenous testosterone production with an exogenous steroid, you will also shut down your natural endogenous estrogen production.Any estrogen production (or lack thereof) would then be derived from whatever exogenous steroids are being administered.This is why some synthetic steroids may not necessarily be as dangerous as we once thought, as the data we use to review their safety profiles are skewed by their lack of estrogenic support in the tissues that would otherwise be supported by testosterone aromatizing into estradiol.In the presence of sufficient estrogen, it is entirely possible that the deleterious effects of certain synthetic steroids in the body may be attenuated to some extent.The Neurotoxicity Of Testosterone, Nandrolone And WinstrolComparing the effect of testosterone with that of 19-nortestosterone (nandrolone) and stanozolol (Winstrol) on neurotoxicity we can clearly see that estrogen is what protects neurons in the brain, not testosterone itself.In this study, a physiologic dosage of testosterone was neuroprotective [R].Testosterone only amplified neurotoxicity at supraphysiological dosages.The neuroprotective effect of a physiologic dosage of testosterone was completely eliminated when the aromatase inhibitor anastrozole (Arimidex) was co-administered, suggesting that the intrinsic toxicity of testosterone as an androgen is only counterbalanced by its aromatization into 17β-estradiol.As opposed to testosterone, nandrolone does not appear to aromatize sufficiently into estrogen, and Winstrol does not interact with aromatase at all.As you would expect, nandrolone and Winstrol were both neurotoxic at every single dose evaluated regardless of Arimidex being co-administered or not.The anti-androgen flutamide was able to attenuate the neurotoxicity of all three androgens, thus further reinforcing that physiologic dosages of androgens without a sufficient amount of opposing estrogens, or supraphysiological dosages of androgens may facilitate neuronal death.None of the anabolic androgenic steroids in this study were toxic in the absence of NMDA, therefore suggesting that the mechanism by which unopposed androgens facilitate neuronal death is by increased vulnerability to excitotoxic insults.TestosteroneNeuroprotective Effect Of Testosterone At Physiologic Dosages Without ArimidexAt physiologic dosages without an aromatase inhibitor present, testosterone has shown to have a neuroprotective effect.Neuroprotective Effect Of Testosterone At Physiologic Dosages Is Eliminated By ArimidexIt is often assumed that the androgen itself (testosterone) is what protects the brain.However, the aromatase inhibitor Arimidex completely eliminated all neuroprotective effects of testosterone at that same physiologic dosage.Arimidex (anastrozole) exacerbated neurotoxicity at every single testosterone dosage when it was co-administered.This suggests that testosterone is not a unique androgen that is more neuroprotective than all other steroids, rather, it is its aromatization into estrogen that is neuroprotective.Neurotoxicity Of Testosterone At Suraphysiological Dosages With And Without ArimidexAt supraphysiological dosages, testosterone has shown to exacerbate neurotoxicity.While its aromatization into estrogen still prevents a significant amount of neuronal death, we can clearly see that supraphysiological testosterone concentrations exacerbate neurotoxicity regardless, and supraphysiological estrogen levels will not provide dose-dependent increases in neuroprotection.What is the takeaway from this?The data suggests that physiologic concentrations of testosterone facilitate neuroprotection in the brain via aromatization into estrogen, but there is a threshold to that neuroprotection, and supraphysiological concentrations will still be unhealthy.Nandrolone (19-nortestosterone)Neurotoxicity Of Nandrolone Regardless Of Arimidex UseNandrolone exacerbated neurotoxicity at all dosages, regardless if it was a low concentration or a high concentration being evaluated.In addition, co-administering Arimidex had no impact on how neurotoxic nandrolone was in this model at any dosage.This suggests that nandrolone does not aromatize into a sufficient amount of estrogen, or activate estrogen receptors on its own at an amount satisfactory to provide the neuroprotective effects of healthy estrogen levels.A source of estrogen would likely be necessary to co-administer with nandrolone for it to be considered a viable monotherapy alternative in a HRT context, or as a “healthy” cycle.Winstrol (Stanozolol)Neurotoxicity Of Winstrol Regardless Of Arimidex UseWinstrol exacerbated neurotoxicity at all dosages, regardless if it was a low concentration or a high concentration being evaluated.In addition, co-administering Arimidex had no impact on how neurotoxic Winstrol was in this model at any dosage.We already know that Winstrol does not aromatize into estrogen at all.This data suggests that a source of estrogen would be necessary to co-administer with Winstrol for it to even be considered as a viable monotherapy alternative in a HRT context, or as a “healthy” cycle.Anti-Androgens Attenuate The Neurotoxicity Of Anabolic Androgenic SteroidsUnopposed androgens with an insufficient amount of estrogen present will be cardiotoxic and neurotoxic.This is why Flutamide (an anti-androgen) was able to eliminate the neurotoxicity of nandrolone and Winstrol.Anti-androgens have a dose-dependent response just like anabolic androgenic steroids, so there will be androgen receptor (AR) competition occurring between anti-androgens and androgens for AR binding and activation.Anti-androgens will act as competitive antagonists for AR, or as makeshift synthetic steroids themselves, albeit with significantly reduced androgenicity.Basically, depending on the anti-androgen used, they will work either by suppressing endogenous androgen production, and/or by competing for androgen receptors.How effective the anti-androgen will be at inhibiting androgens from binding to AR will be based on binding affinity, binding constant, half-life, the dosage used, and a myriad of other factors.Flutamide is non-steroidal and acts as a selective, competitive, silent antagonist of the AR.It is a primitive and subpar anti-androgen relative to more recent developments in medicine, however, it is still effective at preventing androgens from binding to androgen receptors.This is why flutamide was able to eliminate all of the neurotoxicity of nandrolone and Winstrol at all dosages.By preventing nandrolone and Winstrol from binding to androgen receptors, they are no longer able to transcribe their effects in tissues.The flutamide and Arimidex data reinforces the fact that nandrolone does not produce enough estrogen to provide the neuroprotection needed to stave off neuronal death.With or without an aromatase inhibitor, nandrolone exacerbates neurotoxicity just the same.Without an aromatase inhibitor but with an anti-androgen, the neurotoxicity of Nandrolone is eliminated entirely.I suspect that the same applies for the inherent cardiotoxicity of nandrolone as well.Expectedly, the same applies for Winstrol as it is not a substrate for aromatase at all.This is where all the studies showing how terrible nandrolone is for the heart and brain come into question, as those negative outcomes found in the data may not have been so drastic if an exogenous source of estrogen was co-administered.The same dosage of flutamide was unable to fully offset the neurotoxicity of testosterone at supraphysiological dosages without Arimidex present.Once testosterone dosages exceed physiologic concentrations, the vulnerability to neurotoxicity and cardiotoxicity skyrockets.Too much of anything in the body is going to be bad, and testosterone is not exempt from this just because its the bioidentical hormone we naturally produce and aromatize into estrogen.The Aromatization Of Androgens Into Estrogen Is What Regulates NeurotoxicityReflecting on the data with and without an aromatase inhibitor we can see quite clearly that estrogen is what facilitates neuroprotection, not testosterone.Many assume that testosterone is a unique androgen that binds to AR in some special way that’s going to protect the brain and other steroids are going to destroy the brain.I don’t think it’s as cut and dry as that.I think it’s pretty clear in the data that with anastrozole co-administered the neuroprotective effect is wiped out, and without anastrozole there is a neuroprotective effect.What is the difference between aromatase being inhibited and aromatase not being inhibited?It is the estrogen level in the body.If you have a sufficient amount of estrogen to balance out androgens in the body, you get a good stable level of neuroprotection, which is reflected in how our body regulates endogenous androgen aromatization as is.But, if you have a supraphysiological level of androgens, or inhibit aromatase from providing the estrogen needed to carry out necessary functions in the body, neurotoxicity spikes up regardless of the fact that it is testosterone being evaluated, not a non-bioidentical synthetic anabolic steroid.This all circles back to the rationale behind using a testosterone base on cycle, or having a sufficient source of exogenous estrogen if you are deficient.It also reinforces that aromatase inhibitors are horrible for you if used unnecessarily.My Stance On Aromatase InhibitorsYou would be well served by doing whatever you can to avoid using aromatase inhibitors.If you even need an aromatase inhibitor in the first place you’re likely either using too much testosterone to begin with (or other aromatizing steroids), you’re too fat (more fat = more aromatase), your diet sucks, your lifestyle choices are poor, or you’re injecting too infrequently.Or you might have a genetic polymorphism that results in subpar sex hormone metabolism.At the end of the day, the likelihood that you would need an AI to handle a truly therapeutic dose of testosterone if you’ve optimized everything is extremely low.In a bodybuilding context at supraphysiological dosages, I also think that in most cases using an AI just so you can use “too high” of a testosterone dose is a poor strategy.Should You Take Exogenous Estrogen To Prevent Neurotoxicity And CardiotoxicityJust because estrogen is what provides neuroprotection, not testosterone, it absolutely does not mean that you should start popping your girlfriend’s birth control pills like candy.Unopposed estrogen in the body is carcinogenic.There is a reason why the first go to treatments for breast cancer are SERMs and aromatase inhibitors.Also, estrogen does not provide neuroprotection in a dose dependent manner.There is a sweet spot for everything in the body, and too much of anything is going to be bad.A 4-day pretreatment with low concentrations 0.01 μM (10 nM) of 17β-estradiol was substantially neuroprotective against NMDA toxicity.However, you can clearly see that there was not a dose dependent decrease in neurotoxicity in this study.Neuroprotection was significantly lower with 1 μM 17β-estradiol than with the much lower dosage of 0.01 μM 17β-estradiol. More is not better with anything in the body.The body has a tightly regulated system in place whereby a certain amount of estrogen is needed for physiologic functions.Too much estrogen without enough androgens can result in cancer development, gynecomastia (gyno), and a myriad of other issues.Too little estrogen and excessive androgens can result in cardiovascular disease, neuronal death, and a myriad of other issues.So, if you are using an androgen without a sufficient amount of opposing estrogen to balance it out, you will not only be inhibiting muscle growth and fat loss, but you will be putting your body in an even more quickly deteriorating state of health than you would have already been in regardless simply as a result of supraphysiological androgen levels.If you are using a TRT dose of testosterone, you would be best served by not unnecessarily inhibiting aromatase.Also, if you are using an anabolic steroid that is not a potent substrate for aromatase, you would be best served by adding a testosterone base or a source of adequate estrogen to your cycle.The interesting thing to evaluate would be whether all of the anabolic steroids previously described by the literature as horrendous for the heart and brain would still be described as such if an adequate dosage of exogenous estrogen was used in conjunction with them in the corresponding studies.It certainly opens the mind up to potential hormone replacement therapy alternatives, hence my experimentation in the past with Trestolone monotherapy, low dose Nandrolone with exogenous estradiol, and SARMs with exogenous estradiol.Related

Proviron (mesterolone) Bodybuilding Cycle Protocol
Proviron (mesterolone) Bodybuilding Cycle Protocol Proviron. Active: Mesterolone Overview Mesterolone is a synthetic, orally effective androgen which does not have any anabolic characteristics. In the school of medicine they use Mesterolone to ease or cure disturbances caused by a deficiency of male sex hormones. Many athletes believe that using Proviron at the end of a…

Protein and Muscle-Building Research Rundown
One of the most grueling endurance events I’ve ever participated in is the American College of Sports Medicine’s annual meeting. From dawn to dusk every day for nearly a week, scientists present the latest results from their labs. At any given moment, there are at least three presentations that you wish you could see happening…
Kevin Levrone’s Steroid Cycles And How Much Muscle He Gained From Each
Kevin Levrone is among professional bodybuilders like Dorian Yates who have opened up about their steroid cycles and dosages.In an interview with Muscular Development Kevin Levrone outlined his first and second steroid cycles with specific details, which gives us great insight into what kind of compounds and dosages he used to build his physique up.Levrone went through only a handful of cycles before he ended up on the Olympia stage.It’s insane to think that within just a couple years of steroid use Kevin was already standing on stage beside Dorian Yates placing 2nd at the 1992 Mr. Olympia.Kevin Levrone story is one of the best examples in history of elite genetic response to steroids.[embedded content]Kevin Levrone’s First Steroid CycleKevin Levrone started his first steroid cycle at 24 years old, six weeks out of his first competition (the 1990 NPC Maryland State Championship).Kevin first steroid cycle was comprised of:During that went from 198 pounds up to 206 pounds six weeks later while simultaneously burning fat.[embedded content]Although we are only able to have a glimpse of what his physique looks like after that first cycle due to the limited number of available photos, we can get a fair idea of the kind of musculature he was displaying at that first show.When it comes to testosterone use (and steroids in general), an increase in fat-free mass doesn’t necessarily mean that the body weight is comprised of only contractile tissue.This is often overlooked and is evidently exaggerated in the clinical data on graded dose response to testosterone in healthy young men.Because of this, we need to speculate a bit on how much weight Kevin actually gained during this first cycle of actual pure muscle.Based on an 8 pound gain, the simultaneous drop in body fat, and Kevin’s body composition he showed on stage at that first show, we can surmise that he probably gained around 10 pounds of muscle during that 6 week cycle.Kevin Levrone’s Second Steroid CycleAfter winning the 1990 NPC Maryland State Championship, Kevin had some time to eat in a calorie surplus and actually have a full off-season before his next pro qualifier show.Kevin’s second steroid cycle is far more indicative of his genetic response to anabolics as his first cycle was only six weeks long and didn’t have as much leniency in regards to his calorie allotment.Kevin’s second steroid cycle was comprised of:That comes to 1700 mg per AAS per week for his second cycle.Despite that being a fairly aggressive second cycle, Kevin claims he has never experienced negative side effects throughout his entire career.This second cycle is what allowed Kevin to pack on 30 pounds of fat-free mass between 1990 and nationals in 1991.Kevin Levrone’s Contest Prep CycleFor contest prep Kevin would add in androgenic hardening agents and let the more water retensive drugs work out of his system.At the start of contest prep Kevin added in four amps of Winstrol per week, split into twice weekly administration (2 amps administered twice per week).Winstrol V came in 50-milligram amps, so his weekly Winstrol dosage was 200 milligrams.At four weeks out, Kevin dropped the Testosterone, Nandrolone and Anadrol.At two weeks out Kevin added in 20 milligrams per day of Halotestin tabs, and would go into shows on Winstrol and Halo only.Between 1990 and 1991, Kevin’s stage weight increased from 206 pounds to 236 pounds.A 10 pound stage weight increase per year I would consider a VERY successful off-season.[embedded content][embedded content]Kevin managed to put on 30 during his first off-season, and found himself on the Olympia stage placing second to Dorian Yates within 2 years of his first steroid cycle.[embedded content]Related