There’s been a growing amount of hype around the “Deca only cycle”.
While it is most commonly referred to as the Deca only cycle, it is actually based on the compound Nandrolone being used on its own.
The decanoate ester being abbreviated as “Deca” has just become synonymous nowadays in the bodybuilding community with Nandrolone itself.
Seeing the potential merits of Nandrolone as a makeshift hormone replacement therapy alternative to Testosterone, I stopped using Testosterone and instead started using Nandrolone on its own with exogenous Estradiol for 3 months and paid over $1000 for an elaborate blood panel to assess how it affected my health markers.
How Nandrolone Could Potentially Be A Superior HRT Alternative To Testosterone
The primitive thought process is that Nandrolone used in conjunction with Testosterone will lead to horrible side effects, but Nandrolone used on its own will just result in all of the benefits of steroids with a near absence of the androgenic or estrogenic side effects associated with Testosterone use.
In reality, it’s a lot more nuanced than that.
The reason why I found this experiment worth pursuing is the lack of androgenicity of Nandrolone in the body.
Nandrolone 5α-reduces in tissues that express 5α-reductase to the much less androgenic metabolite Dihydronandrolone (DHN).
Nandrolone is basically the only anabolic steroid that is going to maintain 100% anabolic activity of the Nandrolone in muscle tissue where you want it, but also be converted into a much less androgenic metabolite with a lower binding affinity in certain areas of the body where you wouldn’t want Nandrolone to bind.
The two areas of concern for most individuals being hair follicles and skin.
By converting to DHN in these areas, Nandrolone (and by extension DHN) causes less hair loss and acne than Testosterone (and by extension DHT).
In addition, some men are genetically predisposed to high levels of aromatization and estrogen receptor expression and can’t even use TRT doses of Testosterone without experiencing estrogenic side effects.
Nandrolone is not a potent substrate for aromatase, and mainly converts to a weaker estrogen called Estrone (Estradiol is about 10-fold more potent than Estrone).
Nandrolone is also mildly estrogenic on its own via its ability to act as an estrogen receptor alpha (ERα) agonist [R].
Overall, Nandrolone is much less androgenic and estrogenic than Testosterone, and may provide symptom relief in those seeking a viable hormone replacement therapy alternative.
In this context, Nandrolone may also have great potential as an efficacious alternative to Testosterone as an anabolic agent for some individuals who are prone to androgenic and/or estrogenic side effects.
The Neurotoxicity And Cardiotoxicity Of Nandrolone
Based on the limited data available, Nandrolone has shown to be more deleterious to cardiovascular and neurological health than testosterone.
By extrapolating the data, we start to get a clearer picture as to why this likely is.
Nandrolone is mildly estrogenic on its own, and it does not aromatize nearly enough to create as much Estradiol as Testosterone does.
Comparing the effect of testosterone with that of 19-nortestosterone (Nandrolone) and Stanozolol (Winstrol) on neurotoxicity we can clearly see that Estrogen is what protects neurons in the brain, not Testosterone itself.
In this study, a physiologic dosage of Testosterone was neuroprotective [R].
Testosterone only amplified neurotoxicity at supraphysiological dosages.
The neuroprotective effect of a physiologic dosage of Testosterone was completely eliminated when the aromatase inhibitor Anastrozole (Arimidex) was co-administered, suggesting that the intrinsic toxicity of Testosterone as an androgen is only counterbalanced by its aromatization into 17β-estradiol.
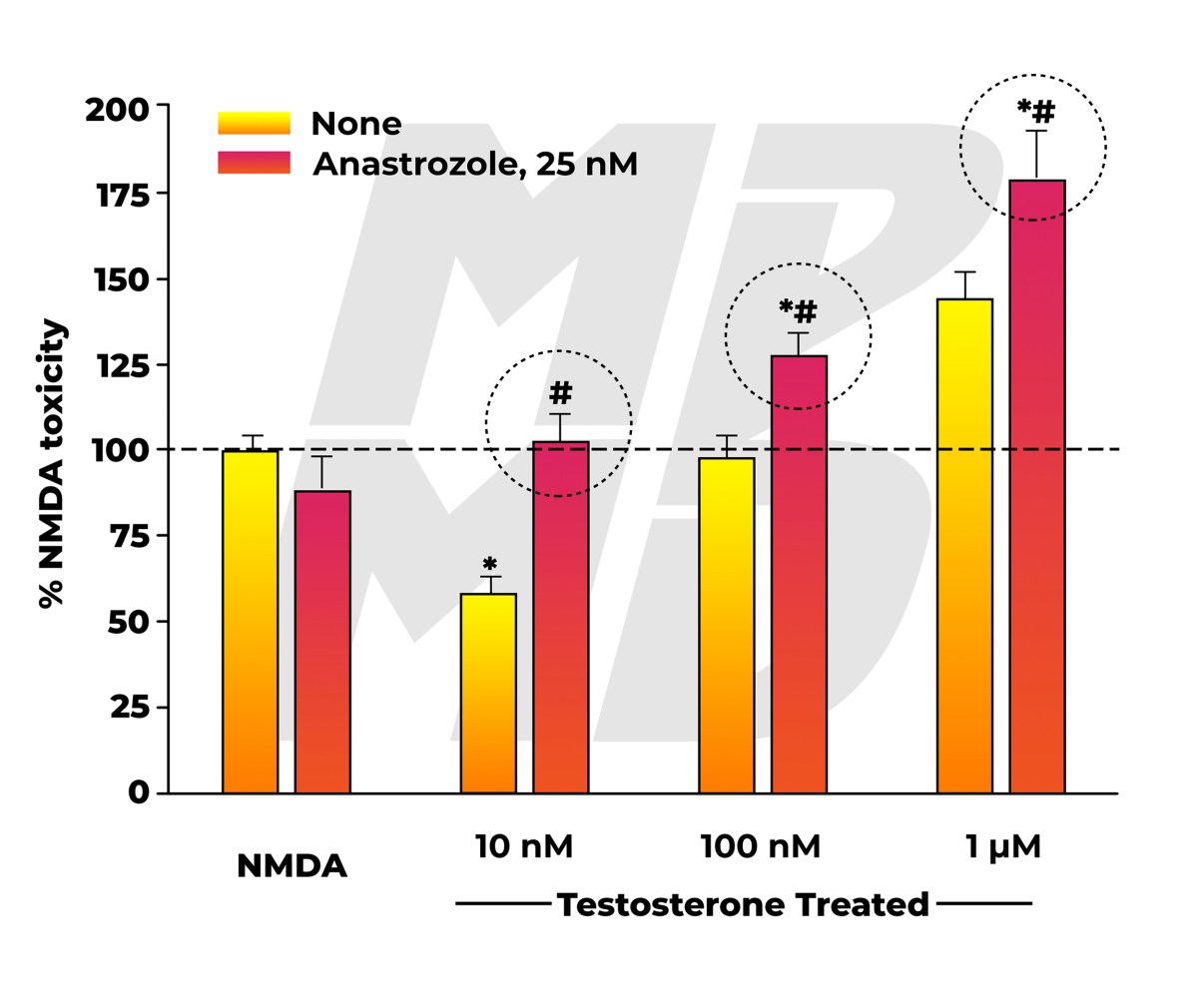

As opposed to testosterone, Nandrolone does not appear to aromatize sufficiently into estrogen.
As you would expect, Nandrolone was neurotoxic at every single dose evaluated regardless of Arimidex being co-administered or not.
If Nandrolone was inherently able to provide enough estrogen receptor alpha (ERα) activation to balance out its androgenicity without even requiring aromatization (it acts as an estrogen on its own to some extent), we would see a neuroprotective effect at equivalent dosages to a physiologic concentration of Testosterone when no AI is used, but that does not appear to be the case either.


The anti-androgen flutamide attenuated the neurotoxicity of all three androgens, thus further reinforcing that physiologic dosages of androgens without a sufficient amount of opposing estrogens, or supraphysiological dosages of androgens may facilitate neuronal death.
I suspect that the same applies for the inherent cardiotoxicity of Nandrolone as well.


Just because you can get your Estradiol levels up to 15 pg/mL with a gram of Deca only, that ratio of androgens to estrogen in the body is way off of what would otherwise be optimal for health based on what I’ve seen.
This is reinforced by the fact that Flutamide (an anti-androgen) was able to attenuate the neurotoxicity of Nandrolone.
By preventing Nandrolone from binding to androgen receptors, it is no longer able to transcribe its effects in tissues.
Hair loss and acne are one thing, cardiotoxicity and neurotoxicity are another thing and should ultimately take precedence obviously.
However, just because Nandrolone monotherapy cannot produce a sufficient ratio of androgens to estrogens, that doesn’t mean that there isn’t a potential loophole.
That loophole is exogenous Estradiol administration.
Exogenous Estradiol Use With Nandrolone Only Cycles
As we’ve seen, Estrogen produced via aromatase is what provides neuroprotection from the androgenicity of Testosterone, not the Testosterone itself.
We also know that Nandrolone is not able to produce enough estrogenic activity in the body to facilitate this same level of neuroprotection.
I theorize that Nandrolone in conjunction with exogenous Estradiol to replace this otherwise missing component could attenuate a significant amount of the deleterious impact Nandrolone has on the heart and brain.
In addition, by providing a sufficient amount of exogenous estrogen, libido, muscle growth, fat loss, and several other aspects of health and performance should be more optimized.
It isn’t a coincidence that cardiovascular disease rates skyrocket once women hit menopause and stop producing Estrogen properly.
The same negative effects will apply in men with low Estrogen levels.
The lack of sufficient Estrogen is often addressed in Deca only cycles by adding an adjunct anabolic steroid that aromatizes into Estrogen or Estrogen analogs.
Obviously for those seeking to minimize androgenic side effects, the ideal way to go about achieving sufficient Estrogen receptor activation is probably not going to be by adding more steroids to their protocol.
This is where exogenous Estradiol comes into play, and I believe the majority of Deca only cycles would be more sustainable from a health perspective, and successful in a bodybuilding context as well with its inclusion.
I have yet to see one person on a Deca only cycle achieve a sufficient Estradiol level relative to their Nandrolone dosage via a sensitive assay Estradiol blood test.
The following blood test result was submitted by an individual on over 1000 mg per week of Deca only.


Over a gram of androgens relative to a 19.2 pg/mL Estradiol level is far from ideal in my opinion.
I had a good conversation with Vigorous Steve as well about his Deca only cycle experience.
He told me that his Estradiol was 12 pg/mL on 1000 mg of Deca per week after 4 weeks, and he ended up adding 25 mg DHEA per day just to bring it up to 25 pg/mL.
When it comes to Nandrolone use on its own, most would benefit from more Estrogen in my opinion.
My Weekly Nandrolone And Estradiol Dosage For “HRT”
Most guys doing Deca only cycles are evaluating Nandrolone at dosages of 600 mg or higher per week for short blasts.
My experiment was based on its potential as an alternative long term HRT option for those prone to androgenic side effects.
Or alternatively, its potential as a compound to swap to periodically throughout the year from TRT to reverse some of the androgenic side effects of Testosterone and DHT while still maintaining the same amount of muscle mass.
Every blood test I’ve seen of Deca only cycle users was on high doses of Nandrolone without a sufficient amount of Estrogen.
I wanted to see how Nandrolone on its own at a “therapeutic dose” would affect my blood work if I had a sufficient amount of Estrogen provided through exogenous Estradiol.
Long-term, the only way Nandrolone monotherapy could be even relatively safe in a cardiovascular context would be with exogenous Estradiol supplementation from what I’ve seen.
And even then, I’m sure it has major drawbacks that will likely accumulate over the years.
With that being said, it is still something I wanted to explore nonetheless, as it is one of the few compounds that can actually support supraphysiological muscle growth with a relatively minimal impact on androgenic alopecia.
Oral micronized Estradiol tablets have quite a few drawbacks.
A few of the most notable drawbacks are that oral Estrogen pills can be somewhat liver toxic, they spike SHBG through the roof, and they result in the production of clotting factors in the blood that do not develop with forms of administration that skip the first pass.
The two most viable methods of administration that skip the first pass are transdermal topical application, or injection.
I chose to topically apply transdermal Estradiol gel (Estrogel) for this experiment.


I used 100 mg of Nandrolone phenylpropionate (NPP) per week split into daily injections using an insulin pin rotating between my glutes and ventroglutes.
I also applied 2.5 grams of transdermal Estrogel (delivering 1.5 mg Estradiol) to my inner thighs every day for over 3 months straight.
Blood Pressure Changes On Nandrolone
One of the first things I noticed was that it was a struggle to keep my blood pressure in check on NPP, even at the mild dose I was using.
What that was caused by exactly, I’m not sure.
I assumed it was Aldosterone prior to this blood work.
When I’m on Testosterone, even when I was using TRT as high as 200 mg per week, I could keep my blood pressure at 110/70 with ease.
Even if I ate terribly, I could still hold 115/75 without even trying on Testosterone.
Within the first week of switching to NPP it became way harder to control my systolic blood pressure.
My diastolic blood pressure was fine for the entire 3 months, but my systolic blood pressure would consistently be around 125-128.
That is not normal for me, and is borderline stage 1 hypertension.
The fact that I even had to try to lower my blood pressure showed to me that Nandrolone is a lot harder to manage in this regard.
This is consistent with almost every single person I know who has blasted high doses of Deca.
They all had significant issues with blood pressure.
Most of the guys who thought they had normal blood pressure were actually stage 1 hypertensive and didn’t even realize that their results were indicative of cardiovascular stress.
My 125-128 systolic occurred without being in a calorie surplus, without any weight changes, and on what I would consider a very low dose of NPP.
The exact same diet, weight, lifestyle, etc. would have me at 110/70 on TRT.
Muscle Growth And Strength On Nandrolone
I maintained my muscle and do not feel that there was a substantial difference between the anabolic potency of Nandrolone compared to Testosterone.
At the very least, the anabolic activity of Nandrolone is comparable to Testosterone, but the androgenic activity is far less than that of Testosterone.
In certain contexts for certain individuals, Nandrolone will be the desirable alternative because of this.
Reduced Libido On Nandrolone – Deca Dick?
My libido was extremely subdued on NPP.
That’s one of the most obvious things I noticed during my experiment.
I had a libido and would still want to have sex, but my libido was much lower than it is on regular TRT.
On TRT I can barely go one day without sex before it starts to consume my mind.
On Nandrolone only, I can easily go a couple days barely even thinking about it.
However, when it came time to get the job done, I could still get the job done and stay hard the entire time without any issues in erection quality.
It was a bit harder to reach orgasm though.
On top of the lack of androgenicity causing a reduction in libido, Nandrolone also has progestogenic activity and binds to the Progesterone receptor.
Excessive Progesterone is notorious for killing libido and causing erectile dysfunction, and it seems that Nandrolone has similar effects in many individuals via this pathway in conjunction with its 5α-reduction into DHN.
My drive was also lower, and I felt less aggressive overall.
In many individuals Testosterone and DHT levels will strongly influence libido, drive, aggression, motivation and productivity.
Personally, even if I have that support via DHT or DHT derivatives, the increased motivation and drive is actually more counterproductive in a work productivity context because my libido gets way too high.
Even when I had high testosterone levels and 0 DHT in my body I still had sex on my mind far more than I would like.
When that happens, I can barely get anything done, and then I end up depleting myself of energy for the day through excessive sex.
The subdued and normalized libido on Nandrolone is welcomed for me because of this.
I don’t think this is necessarily just because I’m a good responder to Nandrolone, I think it has more so to do with the fact that I was using exogenous Estrogen during this experiment with the Nandrolone.
Despite androgens driving aggression and drive, libido and erection quality is largely dictated by adequate Estrogen levels.
With all that being said, DHT (with sufficient Estrogen via Testosterone aromatization) is blatantly better for sexual support than Nandrolone, and testosterone itself, even if you completely inhibited 5α-reductase and nuked DHT, still provides better libido and erection quality than Nandrolone does at equivalent “therapeutic” doses for the majority of people.
My Blood Work Results On A Deca Only Cycle For HRT
I don’t like taking shots in the dark when it comes to something that I see potential in.
There is a lot of theory thrown back and forth in the community on Deca only cycles, and I needed to see for myself how Nandrolone in conjunction with exogenous Estradiol would impact my personal blood work.
I wanted to check markers of oxidative stress, inflammation, kidney function, Aldosterone, Prolactin, hormone levels via sensitive assay testing, and an array of other health markers that are often debated about but very infrequently actually tested for to reinforce statements made.
Expectedly, high dose Deca only cycle blasts will almost always result in low HDL levels, subpar Estradiol levels, and an array of other out of range values that are less common and are more individual dependent.
To date I have yet to see someone get their blood work checked with exogenous Estradiol being used in conjunction with Nandrolone at a “therapeutic” dose.
This is what I wanted to evaluate.
Complete Blood Count with Differential/Platelets
I was actually expecting far worse from my blood test results.
At a “therapeutic” dose, it doesn’t seem like my hematology was negatively affected at all.




Comprehensive Metabolic Panel
In my metabolic panel, nothing was really off to the point that would cause concern.
My BUN being high is likely just the result of being muscular and having a high protein diet.


Lipid Panel
Going into the lipid panel, we can see the number one most common blood test result among steroid users.


My HDL is low.
LDL is also borderline high, but not overly concerning when I can see that my Triglycerides are pretty low.
The reason why my HDL was too low was that my Estrogen levels were too low.
Again, this just reinforces the fact that Nandrolone does not sufficiently aromatize into Estrogen.
I will get into my Estrogen level and why it was still too low even with Estrogel administration later once we get to that part of the blood test results, but my HDL could have been in range if my Estrogen level was in check.
If I didn’t use the Estrogel my HDL likely would have been in the single digits.
I know I can get my HDL into the reference range if my estradiol levels were doubled, which I have the leeway to do.
Iron And Total Iron Binding Capacity
Getting into Iron and TIBC we can see that everything looks pretty normal here.


Total Testosterone And Free Testosterone
Expectedly, by assessing my Total Testosterone level via liquid chromatography with tandem mass spectrometry (LC/MS-MS) and my Free Testosterone level via equilibrium ultrafiltration, we can see that my Testosterone levels were crashed.
Both the total and the free were lower than a healthy female.


This is what you should see in your blood work if you’re on just Nandrolone.
The only Testosterone being produced in my body was indirectly via the trace amounts of androgens produced in my adrenal cortex, which is why the value wasn’t completely bottomed out at 0.
I’ve mentioned many times the importance of getting high sensitivity testing done for hormone levels and how Nandrolone will register as Testosterone in primitive garbage blood tests.
This is another great example of this.
In addition to high sensitivity testing, I had the same blood tested using electrochemiluminescence immunoassay (ECLIA) for my Total Testosterone level, and direct analog enzyme immunoassay (EIA) for my Free Testosterone level.
These were the test results using the exact same blood sample with the terrible default assays that doctors will use to determine how to treat you, and that labs will give you in the majority of your blood work panels.

 According to ECLIA and EIA, I have a normal Total Testosterone and Free Testosterone level.
According to ECLIA and EIA, I have a normal Total Testosterone and Free Testosterone level.
Hilarious.
This just one example of why getting accurate hormone testing is critical.
My Testosterone levels are actually in the gutter, but the stupid primitive tests that doctors and labs give out as defaults for people is so f*cking stupid that it can’t even tell the difference between Testosterone and 19-nortestosterone in my blood.
Renin Activity and Aldosterone
My renin activity and Aldosterone appeared to be normal.


This is one of the main things I wanted to check because there’s a lot of speculation around the effect Nandrolone is going to have on Aldosterone levels.
When it comes to the Deca only cycle, there’s something going on that throws off homeostatic mechanisms that regulate blood pressure that does not appear to be Estrogen related or Aldosterone related.
At least based on my blood work, my Aldosterone was definitely not at a level that could imply any kind of negative effect on blood pressure.
My Aldosterone level was low if anything.
Granted, some markers in the serum can be relatively worthless when compared to actual tissue concentrations, but at least based on my blood work, Aldosterone does not appear to be the culprit.
The first thing many jump to when explaining blood pressure regulation is the effect Nandrolone supposedly has on spiking Aldosterone through the roof, but it just doesn’t appear to be the case in my experience as you can see yourself here.
Vitamin B12 and Folate
My B12 and Folate levels were normal.


Pregnenolone
Pregnenolone appeared to be normal and within the reference range for men which is notable, as many assume that Nandrolone will shut down the production of precursor steroids.
That does not appear to be the case either.
I assumed precursor hormone levels like Pregnenolone would be less affected than many seem to think as most circulating Pregnenolone is derived from the adrenal cortex.


Dihydrotestosterone (DHT)
Expectedly, my DHT was very low.
This is because I have almost no Testosterone being produced to 5α-reduce into DHT.
If my Testosterone is low, my DHT will be low as well.


DHT Backdoor Pathway
Contrary to popular belief, there is a backdoor pathway via Pregnenolone that can create DHT as well, which contributes to the chunk of DHT I have in my blood.


Hemoglobin A1c
Hemoglobin A1c appeared to be normal at 5.1%.


Thyroxine (T4)
My Free T4 was 1.28 ng/dL, which is acceptable.


DHEA-Sulfate
My DHEA was in range and actually on the high end of normal.
Being on exogenous Nandrolone or Testosterone does not shut down DHEA production.


Cortisol
Cortisol was “normal” apparently, although it looks a bit high to me.
I believe this result was mostly sleep hygiene related rather than entirely Nandrolone related.


Thyroid Stimulating Hormone (TSH)
My TSH is too high.
I’ve never had a TSH this high before.
I have had a TSH in the 2’s before, this isn’t the first time, but never this high.


However, based on my resting heart rate and my morning waking temperature and my mid-day temperature, my metabolic rate seems to be the same as it usually is on TRT, and I have had no standout hypothyroidism symptoms.
Luteinizing Hormone (LH) and Follicle Stimulating Hormone (FSH)
Expectedly, LH and FSH were undetectable.


Prolactin
My Prolactin was on the low end of normal.


This was another interesting health marker to see on Nandrolone, as many will often jump to assuming that Nandrolone spikes Prolactin levels through the roof.
That does not appear to be the case though.
Prostate-Apecific Antigen (PSA)
My PSA level was normal, and did not change from my previous blood work on Testosterone for TRT.


D-Dimer
My D-Dimer was normal.
![]()
![]()
A friend of mine had a very high D-Dimer level on a Deca only cycle and he wanted me to check mine to see if there was a pattern.
It looks like the elevated D-Dimer was case-specific for him and was probably caused by something completely unrelated, as my D-Dimer is normal.
C-Reactive Protein
C-Reactive Protein is one of the primary markers we have for assessing inflammation in the body.
A C-Reactive Protein level of 0.34 mg/L is not overly concerning, although I would like to see it below 0.3 mg/L.


I had undetectable C-Reactive Protein levels in the past on TRT, and on Nandrolone it jumped up to 0.34, which is notable.
Estradiol, Sensitive
My Estradiol (E2) level determined via LC/MS-MS was only 15.4 pg/mL, despite administering 2.5 grams of Estrogel per day.


This was disappointing, as I would have liked to see my E2 at least around 30 pg/mL based on the amount of Estrogel I was applying daily.
Evidently, my inner thigh was not absorbing the Estrogel very well.
This is one of the recommended areas of application, but my results were not even close to in line with the average blood levels found in the Estrogel pharmacokinetics studies.
With daily administration of 2.5 g or 5 g Estrogel (corresponding to 1.5 mg or 3 mg estradiol, respectively), mean serum estradiol concentrations of approximately 80 pg/ml (294 pmol/L) and 150 pg/ml (551 pmol/L), respectively, are maintained.
Administration of Estrogel also results in increased serum estrone concentrations, producing a physiological estradiol/estrone ratio of approximately one.
Therefore, serum concentrations of both estradiol and estrone and the serum estradiol/estrone ratio provided by ESTROGEL® are consistent with physiological levels observed during the follicular phase of the normal menstrual cycle.
My inner thigh isn’t very hairy at all as I manscape fairly regularly, so I expected at least a 40 pg/mL E2 based on the amount of Estrogel I was applying.
I was overly generous with my dose based on the off chance that I would encounter an absorption issue, and my E2 was still way below where I expected it to be.
Based on the pharmacokinetics outlined by Merck, 80 pg/mL is the average E2 level for someone applying 2.5 grams of Estrogel per day.
There’s no way I could have predicted that I would have an absorption issue so problematic that it would result in five times lower absorption than the average.
If my E2 was closer to 30 pg/mL, I expect that my HDL would have been pushed into the reference range, and all Estradiol driven physiologic functions likely would have been more optimized.
To me, this just reinforced further that Nandrolone is a subpar source of Estradiol as I was using a high dose of transdermal E2 and still could barely reach a satisfactory E2 level.
To increase my E2 levels for similar future experiments I will either have to find a better application area, add some DMSO to my Estrogel to increase absorption, or consider Estradiol injections instead.
Homocysteine
My Homocysteine level was higher than I would like.


Normally my Homocysteine is closer to 8-8.5 umol/L.
Earlier in the year when I did a shorter Nandrolone experiment for a month using 200 mg per week (double the dose I used for this experiment) I had a Homocysteine level around 8.5, so I doubt this spike was Nandrolone related.
This is one of the main markers I always have my eye on because I am homozygous for the C667T polymorphism.
Gamma-Glutamyl Transferase (GGT)
My GGT looked good.


I was worried that this would be cranked through the roof as it is a marker of oxidative stress.
Magnesium
My magnesium level looked okay.


Copper and Zinc
My zinc level looked okay.
My copper level may be a bit low, which I am now addressing by eating an ounce of beef liver every day.


Progesterone
My Progesterone was normal, which is notable as it is another precursor hormone that many assume drops to zero when exogenous anabolic steroids are present in the body.


Insulin
My insulin level was good.


Estrone
Expectedly, my Estrone was a bit high.


This can be a major problem with exogenous Estradiol and Nandrolone unfortunately.
Estrone Level Increase From Exogenous Estradiol
The ratio of Estrone-to-Estradiol is skewed with massive elevations in Estrone with oral Estrogen administration.
Fortunately, this unhealthy ratio can be avoided for the most part with transdermal Estradiol administration.
High levels of serum Estrone sulfate (E1S) were found after long-term oral estrogen treatment of commonly prescribed dosages, whereas there was a small increase in E1S levels after transdermal Estradiol (E2) therapy.
The mean maximum E1S levels were more than 20-fold higher with oral estradiol (E2) when compared with the 0.05 mg/day transdermal estradiol patch.
This is consistent with the 20-fold higher dose of E2 when compared with the transdermal dose [R].




Estrone Level Increase From Nandrolone
Nandrolone also significantly elevates concentrations of Estrone in plasma [R].


During a pilot study evaluating the possible beneficial effect of Nandrolone Decanoate (ND) on bone metabolism in patients with rheumatoid arthritis there was a significant increase in the serum levels of Estrone [R].

Despite the fact that Estrone can convert to Estradiol, we can clearly see that the amount this actually happens in the body is minimal based on the consistently skewed ratios of androgens to Estradiol in the blood test results of Deca only users (or Nandrolone in general).
Ferritin
My Ferritin level is too low.


This is likely the result of phlebotomizing too frequently in 2019.
Estriol
My Estriol level was undetectable, which was expected.


Triiodothyronine (T3)
My Free T3 level was 2.7 pg/mL.


It’s not low enough for me to be overly concerned, however, it is suboptimal and should be in the low 3’s at least.
This is something I will need to address moving forward.
With that being said, I like to look at my resting heart rate as well as my body temperature for a more accurate assessment of my metabolism, and both are where I want them to be.
My waking temperature has consistently been 98 degrees Fahrenheit, and my midday temperature has consistently been 98.6 degrees Fahrenheit.
Sex Hormone-Binding Globulin
Expectedly, my sex hormone-binding globulin (SHBG) was low.


While this isn’t as relevant for a Nandrolone only user as Nandrolone has a very low affinity for SHBG, this is a value I would still like to see in the reference range, especially if I was on TRT.
If I had the Estradiol level I was shooting for, I’m confident that my SHBG would have been in the reference range.
My Overall Experience On Nandrolone And Exogenous Estrogen For HRT
I was expecting to see a bunch of red flags in my blood work, but nothing really stood out as a major concern to me except for the spike in systolic blood pressure, and the high Estrone level.
A before and after echocardiogram and calcium scoring would have been nice to see, but unfortunately I can only afford to do so much in these experiments, and the blood work was expensive enough as is.
I felt good throughout the entire experiment, I maintained my physique, my libido and penis were functional, and my blood work looked pretty good considering that each issue was something more so related to my Estradiol administration than the Nandrolone itself.
Estrone being out of range is a concern, as I would need to use even more exogenous Estradiol to achieve what I would consider a more therapeutic E2 level, which would likely push my Estrone up even higher.
The difficulty in controlling the blood pressure spike is also a huge concern and could be a deal breaker.
If I gave this experiment more time, it is entirely possible that certain things would have become problematic that appeared to be fine during my three month assessment, like my libido or sense of well-being.
It is also possible that despite maintaining a healthy Estrogen level, the same neurological and cardiovascular issues we see in a significant amount of the Nandrolone data could still accumulate over time.
In addition, healthy looking serum levels of Estradiol may not necessarily reflect adequate localized Estrogen receptor activation in each tissue.
With Testosterone, there is a regulated amount of aromatization occurring in each tissue to satisfy however much Estrogen receptor (ER) activation we need.
In the context of Deca only cycles, or Nandrolone monotherapy, there’s nothing else I can refer to other than serum levels, my libido, sense of well-being, other cardiovascular health markers, etc.
In other words, just because you feel good and your Estrogen levels look good on paper, that doesn’t mean that an exogenously administered source of Estrogen is providing the same therapeutic ER activation in all tissues like it would if it were regulated via aromatase.
With that being said, you could also argue the opposite as adequate receptor activation via exogenous hormone therapy is essentially all HRT boils down to to begin with in the context of any hormone.
More than 95% of our endogenous Testosterone is produced in the testes.
Testosterone is supplied to target tissues in the blood, just like most other hormones in the body.
If you inject exogenous Testosterone, it then goes into the blood and is supplied to target tissues.
If you inject anything it goes into the blood and then is carried to the areas that it is needed.
Estrogen replacement has been deemed satisfactory for fulfilling the same functions as endogenously produced Estrogen in women for years, and synthetic Estrogen analogs are handed out like candy to millions of young girls (including teenagers).
Is it healthy?
Estrogen analogs like Ethinyl Estradiol probably aren’t ideal for regulating Estrogen dependent functions, and they definitely aren’t ideal for developing women who haven’t fully matured.
However, there is tons of data to support the fact that exogenous Estradiol is well-tolerated, has a strong safety profile, and can still fulfill physiologic functions sufficiently.
In an ideal world, this would be a regulated process in the body in each tissue (aromatization).
My experiments do not necessarily reflect what I believe are best practice with these hormones, which should be noted.
This was an experiment, and not something that I would recommend someone else do.
Using an exogenous progestogen with estrogel certainly isn’t what I would consider an optimal HRT protocol, or what is indicative of an ideal means of providing androgenic and estrogenic support in tissues.
With that being said, I don’t see a better way to go about utilizing Nandrolone on its own for HRT.
Should it even be considered as an HRT alternative though?
That’s the question, and I believe it is largely going to be individual dependent, with a significant amount of users having poor outcomes in one aspect or another.
I do believe there are a minority of individuals who are very prone to androgenic and/or estrogenic side effects from exogenous Testosterone use that may benefit from exploring Nandrolone though, and it should not be discarded as a potentially viable alternative simply because it is not the primary bioidentical hormone that men produce.