


Area 1255
New member
HYPO Prolactinemia, a cause for concern or ideal state?
Bodybuilders, Fitness Enthusiasts and ordinary men who have had elevated prolactin know firsthand the downsides of High Prolactin levels; it will ruin your sex drive, decrease testosterone production as well as dopamine and turn you into an Apathetic and passive zombie. In the meantime, you are gaining weight and suffering from insulin resistance. So we know for sure that high Prolactin is bad, but do we know the whole story behind prolactin's effects? Moreover, when people go on dopaminergics to lower prolactin back into the normal range, some actually end up nearly obliterating prolactin. As the level of prolactin fades into the deficient or even undetectable stage, should we be worried of possible side-effects? There is a condition describing this stage, it's called HypoProlactinaemia (as opposed to Hyperprolactinaemia which describes high prolactin), and it can also present serious side-effects.
Let's start by defining the effects of prolactin on the androgen receptor, according to PubMed - prolactin increases androgen uptake in the Prostate and also increases 5-Alpha-Reductase (the enzyme that converts testosterone into DHT).
Prostate. 1988;12(3):221-9.
Prolactin effect on the permeability of human benign hyperplastic prostate to testosterone.
Farnsworth WE.
Abstract
While it has been known for over 30 years that prolactin (Prl) synergizes with androgen in the support and stimulation of prostatic growth and metabolism, the evidence that this is accomplished through increasing access of the steroid to the cellular machinery of the gland has arisen only since about 1970. There is widespread uncertainty as to how the Prl effect takes place: by 1) increasing the free steroid concentration in the blood; 2) facilitating the uptake of protein-bound androgen; 3) increasing, by metabolism or receptor-binding, the concentration gradient that can support passive diffusion of the steroid across the plasma membrane; or 4) modification of the fluidity of the membrane itself to increase the solubility of the steroid in the lipoprotein and, thus, the ease of penetration of the cell. The present study attempted to learn if Prl is an effective stimulus of androgen uptake when the first three options are not operative. Using an equilibrium exchange procedure to track the uptake of [17 alpha-3H]-testosterone ([17 alpha-3H]-T) into minced benign hyperplastic human prostate tissue and the irreversible metabolism of the entering steroid to [17 alpha-3H]-dihydrotestosterone [17 alpha-3H]-DHT, it was found that the rate of production of the 5 alpha-reduced metabolite, during a 1-hr incubation in vitro, was directly proportional to the concentration of ovine Prl over the dose range of 0-160 ng/ml. The clinical significance of Prl mediation of steroid uptake is discussed, and suggestions are made as to how the Prl might alter the permeability of the plasma membrane.
PMID: 2453860 [PubMed - indexed for MEDLINE]
Prolactin also has a DIRECT effect on Adrenal Androgen release; being synergistic with ACTH in increasing androgen output (starting with DHEA).(1)
Therefore one would assume that by lowering prolactin excessively, one would then enter a Hypoandrogenic state or at the least a state of 5-alpha-reductase deficiency. This makes sense being that yet another study showed a group of males with induced low prolactin - were rendered infertile with oligozoospermia, asthenospermia, and hypofunction of seminal vesicles(2). DHT has known effects on maintaining normal sperm motility and production as well as stimulating both seminal vesicles and allowing for normal ejaculation(3)(4).
Therefore, we are describing hypoprolactinaemia as a state similar to the 5-AR deficiency in users of the 5-AR inhibiting drug Finasteride.
Arch Androl. 1989;23(3):259-65.
Hypoprolactinemia as related to seminal quality and serum testosterone. Gonzales GF1, Velasquez G, Garcia-Hjarles M. Author information Abstract Semen quality and serum testosterone were studied in six men with hypoprolactinemia (less than or equal to 6 ng/ml) and in normoprolactinemic controls. The incidence of hypoprolactinemia in 92 men attending an infertility clinic was 7.5%. Males with hypoprolactinemia showed in high percentage of disorders (oligozoospermia, 50%; asthenospermia, 75%; hypofunction of seminal vesicles, 67%; and hypoandrogenism, 67%). Hypoprolactinemia is a clinical disorder associated mainly with poor sperm motility.
PMID:
2619414
[PubMed - indexed for MEDLINE]
One other study also described the side-effects of low prolactin in men even better; men presented with Metabolic Syndrome, Premature Ejaculation, Anxiety and Ateriogenic Erectile Dysfunction(5). With this picture, it is looking like low prolactin is causing not only androgen deficiency (or at least low DHT) but also some sort of haywire nervous system....anxiety and premature ejaculation both are associated with elevated glutamate and possibly norpinephrine.
So I went even further and found these studies.
The effect of prolactin on glutamate decarboxylase activity and GABA concentration in hypothalamic slices.
B H Duvilanski, A Seilicovich, M C Diaz, M Lasaga, L Debeljuk Centro de Investigaciones en Reproduction, Facultad de Medicina, Universidad de Buenos Aires, 1121 Buenos Aires, Argentina Psychoneuroendocrinology
(Impact Factor: 5.14). 02/1987; 12(2):107-16. DOI:10.1016/0306-4530(87)90041-2
PubMed ABSTRACT
The effect of prolactin on the activity of GABA-related enzymes and GABA concentrations were studied in hypothalamic slices incubated in vitro. After short periods of incubation (up to 40 min), prolactin (0.25 micrograms/ml) added to the incubation medium produced a significant increase (21% at 20 min of incubation) in glutamic acid decarboxylase (GAD) activity in the hypothalamic slices. A higher concentration of prolactin (1.0 micrograms/ml) produced a slight but significant decrease (8% at 20 min of incubation) in hypothalamic GAD activity. However, after longer periods of incubation (over 8 hr), both doses of prolactin induced a sustained increase in hypothalmic GAD activity, a response which depends upon protein synthesis. No changes were observed in GABA-transaminase (GABA-T) activity of hypothalamic slices incubated in the presence of prolactin. Prolactin decreased GABA concentration in the hypothalami incubated for 10 hr and, at the same time, increased GABA release into the medium. These results indicate that prolactin modifies the synthesis and release of hypothalmic GABA and suggest the existence of a feedback mechanism that prolactin may exert directly at the hypothalamic level.
Neuroscience. 2002;114(1):229-38.
Prolactin-releasing peptide (PrRP) promotes awakening and suppresses absence seizures.
Lin SH1, Arai AC, España RA, Berridge CW, Leslie FM, Huguenard JR, Vergnes M, Civelli O.
Abstract
Prolactin releasing peptide (PrRP) is a recently identified neuropeptide that stimulates prolactin release from pituitary cells. The presence of its receptor outside the hypothalamic-pituitary axis suggests that it may have other functions. We present here evidence that PrRP can modulate the activity of the reticular thalamic nucleus, a brain region with prominent PrRP receptor expression that is critical for sleep regulation and the formation of non-convulsive absence seizures. Intracerebroventricular injection of PrRP (1-10 nmol) into sleeping animals significantly suppresses sleep oscillations and promotes rapid and prolonged awakening. Higher concentrations of PrRP (10-100 nmol) similarly suppress spike wave discharges seen during absence seizures in genetic absence epilepsy rats from Strasbourg, an animal model for this disorder. In concordance with these findings, PrRP suppressed evoked oscillatory burst activity in reticular thalamic slices in vitro. These results indicate that PrRP modulates reticular thalamic function and that activation of its receptor provides a new target for therapies directed at sleep disorders and absence seizures.
Given both of these studies dictate prolactin as inhibitory, we can conclude that prolactin may be protective against excessive glutamate by increasing the enzymes that Convert glutamate into GABA (the brains primary inhibitory or "calming" neurotransmitter). Then this makes sense as well, since glutamate generally increases prolactin, whereas GABA inhibits prolactin, low prolactin then increases glutamate in order to try and raise prolactin up to the norm - by negative feedback. Unfortunately, in many cases this particular adaptation response fails, because the low prolactin state is often induced by drugs or bulimia.
This also makes sense going back to the other study showing hypoprolactinaemia as causing anxiety and premature ejactulation, as said before (and my theory was correct), glutamate excess or deficiency of GABA becomes apparent when prolactin drops too low. Therefore seizure disorders, anxiety, OCD and other similar disorders may also appear in the presence of low prolactin.
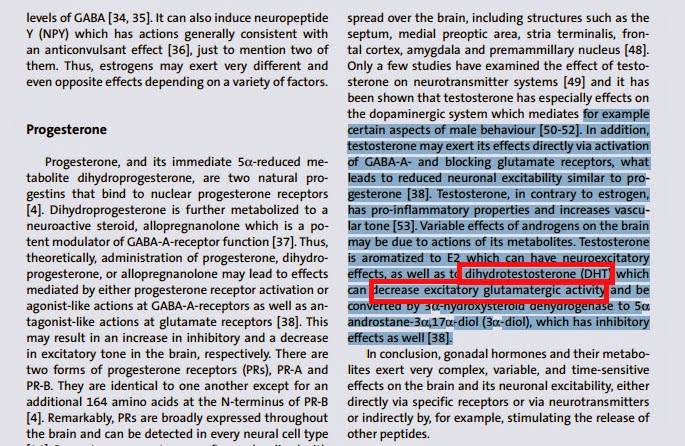
Considering Androgens such as DHT also increase GABA release while decreasing glutamate, and that low prolactin levels lead to low androgen or at least low DHT - this represents another mechanism by which hypoprolactinaemia (low prolactin) causes anxiety and restlessness.
Therefore in Summary, HypoProlactinaemia (though decreasing or eliminating the refractory period) may be outweighed by the other side-effects of low prolactin and so I advise caution against reducing prolactin to a deficient or undetectable state, especially in those particularly susceptible to anxiety, E.D, or any like conditions.
Deficient Prolactin in men induces low DHT levels and lower Androgen levels.
Low Prolactin may cause anxiety; by decreasing GABA synthesis and increasing glutamate activity.
Low Prolactin may cause Calcium Channel overload and increased noradrenaline.
Low Prolactin may cause male infertility; oligozoospermia and asthenospermia.
Hypoprolactinaemia also leads to premature ejaculation and anxiety induced and / or arteriogenic E.D.
Bodybuilders, Fitness Enthusiasts and ordinary men who have had elevated prolactin know firsthand the downsides of High Prolactin levels; it will ruin your sex drive, decrease testosterone production as well as dopamine and turn you into an Apathetic and passive zombie. In the meantime, you are gaining weight and suffering from insulin resistance. So we know for sure that high Prolactin is bad, but do we know the whole story behind prolactin's effects? Moreover, when people go on dopaminergics to lower prolactin back into the normal range, some actually end up nearly obliterating prolactin. As the level of prolactin fades into the deficient or even undetectable stage, should we be worried of possible side-effects? There is a condition describing this stage, it's called HypoProlactinaemia (as opposed to Hyperprolactinaemia which describes high prolactin), and it can also present serious side-effects.
Let's start by defining the effects of prolactin on the androgen receptor, according to PubMed - prolactin increases androgen uptake in the Prostate and also increases 5-Alpha-Reductase (the enzyme that converts testosterone into DHT).
Prostate. 1988;12(3):221-9.
Prolactin effect on the permeability of human benign hyperplastic prostate to testosterone.
Farnsworth WE.
Abstract
While it has been known for over 30 years that prolactin (Prl) synergizes with androgen in the support and stimulation of prostatic growth and metabolism, the evidence that this is accomplished through increasing access of the steroid to the cellular machinery of the gland has arisen only since about 1970. There is widespread uncertainty as to how the Prl effect takes place: by 1) increasing the free steroid concentration in the blood; 2) facilitating the uptake of protein-bound androgen; 3) increasing, by metabolism or receptor-binding, the concentration gradient that can support passive diffusion of the steroid across the plasma membrane; or 4) modification of the fluidity of the membrane itself to increase the solubility of the steroid in the lipoprotein and, thus, the ease of penetration of the cell. The present study attempted to learn if Prl is an effective stimulus of androgen uptake when the first three options are not operative. Using an equilibrium exchange procedure to track the uptake of [17 alpha-3H]-testosterone ([17 alpha-3H]-T) into minced benign hyperplastic human prostate tissue and the irreversible metabolism of the entering steroid to [17 alpha-3H]-dihydrotestosterone [17 alpha-3H]-DHT, it was found that the rate of production of the 5 alpha-reduced metabolite, during a 1-hr incubation in vitro, was directly proportional to the concentration of ovine Prl over the dose range of 0-160 ng/ml. The clinical significance of Prl mediation of steroid uptake is discussed, and suggestions are made as to how the Prl might alter the permeability of the plasma membrane.
PMID: 2453860 [PubMed - indexed for MEDLINE]
Prolactin also has a DIRECT effect on Adrenal Androgen release; being synergistic with ACTH in increasing androgen output (starting with DHEA).(1)
Therefore one would assume that by lowering prolactin excessively, one would then enter a Hypoandrogenic state or at the least a state of 5-alpha-reductase deficiency. This makes sense being that yet another study showed a group of males with induced low prolactin - were rendered infertile with oligozoospermia, asthenospermia, and hypofunction of seminal vesicles(2). DHT has known effects on maintaining normal sperm motility and production as well as stimulating both seminal vesicles and allowing for normal ejaculation(3)(4).
Therefore, we are describing hypoprolactinaemia as a state similar to the 5-AR deficiency in users of the 5-AR inhibiting drug Finasteride.
Arch Androl. 1989;23(3):259-65.
Hypoprolactinemia as related to seminal quality and serum testosterone. Gonzales GF1, Velasquez G, Garcia-Hjarles M. Author information Abstract Semen quality and serum testosterone were studied in six men with hypoprolactinemia (less than or equal to 6 ng/ml) and in normoprolactinemic controls. The incidence of hypoprolactinemia in 92 men attending an infertility clinic was 7.5%. Males with hypoprolactinemia showed in high percentage of disorders (oligozoospermia, 50%; asthenospermia, 75%; hypofunction of seminal vesicles, 67%; and hypoandrogenism, 67%). Hypoprolactinemia is a clinical disorder associated mainly with poor sperm motility.
PMID:
2619414
[PubMed - indexed for MEDLINE]
One other study also described the side-effects of low prolactin in men even better; men presented with Metabolic Syndrome, Premature Ejaculation, Anxiety and Ateriogenic Erectile Dysfunction(5). With this picture, it is looking like low prolactin is causing not only androgen deficiency (or at least low DHT) but also some sort of haywire nervous system....anxiety and premature ejaculation both are associated with elevated glutamate and possibly norpinephrine.
So I went even further and found these studies.
The effect of prolactin on glutamate decarboxylase activity and GABA concentration in hypothalamic slices.
B H Duvilanski, A Seilicovich, M C Diaz, M Lasaga, L Debeljuk Centro de Investigaciones en Reproduction, Facultad de Medicina, Universidad de Buenos Aires, 1121 Buenos Aires, Argentina Psychoneuroendocrinology
(Impact Factor: 5.14). 02/1987; 12(2):107-16. DOI:10.1016/0306-4530(87)90041-2
PubMed ABSTRACT
The effect of prolactin on the activity of GABA-related enzymes and GABA concentrations were studied in hypothalamic slices incubated in vitro. After short periods of incubation (up to 40 min), prolactin (0.25 micrograms/ml) added to the incubation medium produced a significant increase (21% at 20 min of incubation) in glutamic acid decarboxylase (GAD) activity in the hypothalamic slices. A higher concentration of prolactin (1.0 micrograms/ml) produced a slight but significant decrease (8% at 20 min of incubation) in hypothalamic GAD activity. However, after longer periods of incubation (over 8 hr), both doses of prolactin induced a sustained increase in hypothalmic GAD activity, a response which depends upon protein synthesis. No changes were observed in GABA-transaminase (GABA-T) activity of hypothalamic slices incubated in the presence of prolactin. Prolactin decreased GABA concentration in the hypothalami incubated for 10 hr and, at the same time, increased GABA release into the medium. These results indicate that prolactin modifies the synthesis and release of hypothalmic GABA and suggest the existence of a feedback mechanism that prolactin may exert directly at the hypothalamic level.
Neuroscience. 2002;114(1):229-38.
Prolactin-releasing peptide (PrRP) promotes awakening and suppresses absence seizures.
Lin SH1, Arai AC, España RA, Berridge CW, Leslie FM, Huguenard JR, Vergnes M, Civelli O.
Abstract
Prolactin releasing peptide (PrRP) is a recently identified neuropeptide that stimulates prolactin release from pituitary cells. The presence of its receptor outside the hypothalamic-pituitary axis suggests that it may have other functions. We present here evidence that PrRP can modulate the activity of the reticular thalamic nucleus, a brain region with prominent PrRP receptor expression that is critical for sleep regulation and the formation of non-convulsive absence seizures. Intracerebroventricular injection of PrRP (1-10 nmol) into sleeping animals significantly suppresses sleep oscillations and promotes rapid and prolonged awakening. Higher concentrations of PrRP (10-100 nmol) similarly suppress spike wave discharges seen during absence seizures in genetic absence epilepsy rats from Strasbourg, an animal model for this disorder. In concordance with these findings, PrRP suppressed evoked oscillatory burst activity in reticular thalamic slices in vitro. These results indicate that PrRP modulates reticular thalamic function and that activation of its receptor provides a new target for therapies directed at sleep disorders and absence seizures.
Given both of these studies dictate prolactin as inhibitory, we can conclude that prolactin may be protective against excessive glutamate by increasing the enzymes that Convert glutamate into GABA (the brains primary inhibitory or "calming" neurotransmitter). Then this makes sense as well, since glutamate generally increases prolactin, whereas GABA inhibits prolactin, low prolactin then increases glutamate in order to try and raise prolactin up to the norm - by negative feedback. Unfortunately, in many cases this particular adaptation response fails, because the low prolactin state is often induced by drugs or bulimia.
This also makes sense going back to the other study showing hypoprolactinaemia as causing anxiety and premature ejactulation, as said before (and my theory was correct), glutamate excess or deficiency of GABA becomes apparent when prolactin drops too low. Therefore seizure disorders, anxiety, OCD and other similar disorders may also appear in the presence of low prolactin.
Considering Androgens such as DHT also increase GABA release while decreasing glutamate, and that low prolactin levels lead to low androgen or at least low DHT - this represents another mechanism by which hypoprolactinaemia (low prolactin) causes anxiety and restlessness.
Therefore in Summary, HypoProlactinaemia (though decreasing or eliminating the refractory period) may be outweighed by the other side-effects of low prolactin and so I advise caution against reducing prolactin to a deficient or undetectable state, especially in those particularly susceptible to anxiety, E.D, or any like conditions.
Deficient Prolactin in men induces low DHT levels and lower Androgen levels.
Low Prolactin may cause anxiety; by decreasing GABA synthesis and increasing glutamate activity.
Low Prolactin may cause Calcium Channel overload and increased noradrenaline.
Low Prolactin may cause male infertility; oligozoospermia and asthenospermia.
Hypoprolactinaemia also leads to premature ejaculation and anxiety induced and / or arteriogenic E.D.
Last edited:
