

[h=2]
 There are three different PPAR isoforms:
There are three different PPAR isoforms:
 Note: Macrophages are cells that are responsible for the elimination of disease-causing germs, dead cells and cellular debris.
Note: Macrophages are cells that are responsible for the elimination of disease-causing germs, dead cells and cellular debris.
PPAR-alpha activation increases the expression of lipoprotein lipase and apolipoprotein A-V (apoA-V) and decreases the expression of apoC-III in the liver. This decreases LDL particles (bad cholesterol), decreases blood triglycerides levels and liberates fatty acids, allowing them to be oxidized (burned).Note: LDL stands for low density lipoprotein and is often referred to as bad cholesterol. HDL stands for high density lipoprotein and if often referred to as good cholesterol.
Note 2: A lipase is an enzyme that helps break down fats into glycerol and fatty acids.
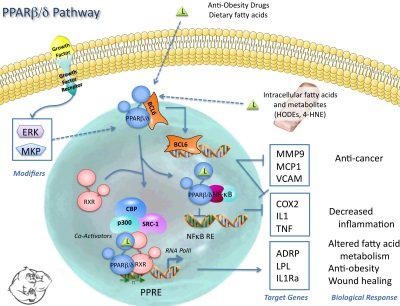
In addition, PPAR-alpha activation increases hepatic apoA-I andapoA-II, which increasing HDL levels (good cholesterol).PPAR-alpha activation increases fat loss and improves cholesterol levels by lowering LDL levels, decreasing blood triglycerides and increasing HDL levels.[h=2]PPAR-beta/delta[/h]The exact actions of PPAR-beta/delta (β/ δ) in humans are still being researched. Animal studiesshow that PPAR-beta/delta activation decreases adiposity tissue (body fat). Most researchers speculate that PPAR-beta/delta acts similarly to PPAR-alpha but has more specific actions in skeletal muscle, in both humans and animals.[h=2]PPAR-Gamma[/h]PPAR-gamma is found primarily in adipocytes (fat cells), vascular endothelium, vascular smooth muscle, and macrophages. It is involved in the storage of fatty acids and is activated by leukotrienes, prostaglandins, and fatty acids.
 Note: Leukotrienes are a group of compounds derived from arachidonic acid that participate in inflammatory reactions.
Note: Leukotrienes are a group of compounds derived from arachidonic acid that participate in inflammatory reactions.
Note: Prostaglandins are hormone-like compounds produced in body tissue that regulate blood pressure, smooth muscle activity, inflammation, calcium movement, hormone regulation, and cell growth control.
Activation of PPAR-gamma will increase the transcription of genes and enzymes involved in insulin sensitivity and decrease their activity in adipogenesis (fat cell creation) and the inflammatory process.Obesity and insulin resistance suppress PPAR-gamma activation. Activation of PPAR-gamma could theoretically cure type 2 diabetes. The anti-diabetic drug thiazolidinediones has been successfully used to treat type-2 diabetes in human clinical trials through its role in activating PPAR-gamma, though hepatoxicity and risk of congestive heart failure discontinued the research on the drug.[h=2]Cardarine[/h]Cardarine (also known as GW501516) is a PPAR receptor agonist invented by Ligand Pharmaceuticals and GlaxoSmithKline in the 1990s. Cardarine was developed to treat obesity, diabetes, lipid strain, and cardiovascular diseases. Those who run blood work when using cardarine will notice that their cholesterol levels will improve substantially.In 2007 research was published showing that mice given GW501516 had dramatically improved physical performance which popularized the drug as a doping agent. The World Anti-Doping Agency (WADA) added GW501516 to the prohibited list in 2009.Side effects are rare with cardarine. Since cardarine is non hormonal, there is no need to worry about PCT or hormone suppression. The recommended dose for both men and women is 10-20 milligrams (mg) per day.The half-life of cardarine is 20-24 hours, meaning that a once per day dose is all that is needed.[h=2]SARMS[/h]Selective Androgen Receptor Modulators (SARMs) are a class of therapeutic compounds that have similar properties to steroids, but with reduced androgenic properties. There is a misconception floating around that SARMS are completely anabolic substances and carry no androgenic properties. That is not technically true as SARMS do possess some androgenic properties and have a high binding affinity for the androgen receptor. However, the androgenic properties of SARMS are so minimal that they are pretty much negligible. Even the most androgenic SARM, Testolone (RAD140), has only one tenth the androgenic properties of testosterone.The main difference between SARMS and steroids is that SARMS act in a very targeted way and are very selective in their mechanisms of action. SARMS have a special affinity for certain tissues like muscle and bone, but not for other tissues like the prostate, liver, and brain. They also don’t convert into unwanted molecules that cause side effects, like DHT and estrogen. This makes side effects associated with steroid usage like gynecomastia (gyno), water retention, hair loss etc. impossible with SARM usage.Some SARMS will suppress natural testosterone production and HPTA function but their rate of suppression is minimal, and a mini post cycle therapy (PCT) with a good natural testosterone booster is all that is needed after a cycle of SARMS.
A deep explanation why PPAR agonists are NOT SARMS....
Summary:
- PPAR agonists possess no anabolic activity and do no bind to the androgen receptor
- PPAR agonists do not suppress HPTA or effect testosterone production in any way
- PPAR agonists increase endurance but carry no stimulant nature so they will not affect sleep or cortisol levels
Fig 1. PPAR Layout
- Alpha (α)
- Beta/delta (β/ δ)
- Gamma (γ)
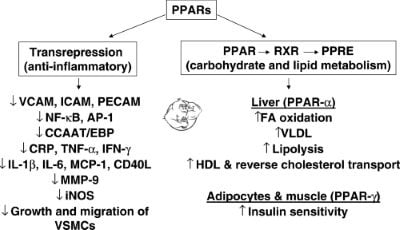
Fig 2. PPAR Alpha/Gamma
PPAR-alpha activation increases the expression of lipoprotein lipase and apolipoprotein A-V (apoA-V) and decreases the expression of apoC-III in the liver. This decreases LDL particles (bad cholesterol), decreases blood triglycerides levels and liberates fatty acids, allowing them to be oxidized (burned).Note: LDL stands for low density lipoprotein and is often referred to as bad cholesterol. HDL stands for high density lipoprotein and if often referred to as good cholesterol.
Note 2: A lipase is an enzyme that helps break down fats into glycerol and fatty acids.
In addition, PPAR-alpha activation increases hepatic apoA-I andapoA-II, which increasing HDL levels (good cholesterol).PPAR-alpha activation increases fat loss and improves cholesterol levels by lowering LDL levels, decreasing blood triglycerides and increasing HDL levels.[h=2]PPAR-beta/delta[/h]The exact actions of PPAR-beta/delta (β/ δ) in humans are still being researched. Animal studiesshow that PPAR-beta/delta activation decreases adiposity tissue (body fat). Most researchers speculate that PPAR-beta/delta acts similarly to PPAR-alpha but has more specific actions in skeletal muscle, in both humans and animals.[h=2]PPAR-Gamma[/h]PPAR-gamma is found primarily in adipocytes (fat cells), vascular endothelium, vascular smooth muscle, and macrophages. It is involved in the storage of fatty acids and is activated by leukotrienes, prostaglandins, and fatty acids.
Fig 3. PPAR Beta Pathway
Note: Prostaglandins are hormone-like compounds produced in body tissue that regulate blood pressure, smooth muscle activity, inflammation, calcium movement, hormone regulation, and cell growth control.
Activation of PPAR-gamma will increase the transcription of genes and enzymes involved in insulin sensitivity and decrease their activity in adipogenesis (fat cell creation) and the inflammatory process.Obesity and insulin resistance suppress PPAR-gamma activation. Activation of PPAR-gamma could theoretically cure type 2 diabetes. The anti-diabetic drug thiazolidinediones has been successfully used to treat type-2 diabetes in human clinical trials through its role in activating PPAR-gamma, though hepatoxicity and risk of congestive heart failure discontinued the research on the drug.[h=2]Cardarine[/h]Cardarine (also known as GW501516) is a PPAR receptor agonist invented by Ligand Pharmaceuticals and GlaxoSmithKline in the 1990s. Cardarine was developed to treat obesity, diabetes, lipid strain, and cardiovascular diseases. Those who run blood work when using cardarine will notice that their cholesterol levels will improve substantially.In 2007 research was published showing that mice given GW501516 had dramatically improved physical performance which popularized the drug as a doping agent. The World Anti-Doping Agency (WADA) added GW501516 to the prohibited list in 2009.Side effects are rare with cardarine. Since cardarine is non hormonal, there is no need to worry about PCT or hormone suppression. The recommended dose for both men and women is 10-20 milligrams (mg) per day.The half-life of cardarine is 20-24 hours, meaning that a once per day dose is all that is needed.[h=2]SARMS[/h]Selective Androgen Receptor Modulators (SARMs) are a class of therapeutic compounds that have similar properties to steroids, but with reduced androgenic properties. There is a misconception floating around that SARMS are completely anabolic substances and carry no androgenic properties. That is not technically true as SARMS do possess some androgenic properties and have a high binding affinity for the androgen receptor. However, the androgenic properties of SARMS are so minimal that they are pretty much negligible. Even the most androgenic SARM, Testolone (RAD140), has only one tenth the androgenic properties of testosterone.The main difference between SARMS and steroids is that SARMS act in a very targeted way and are very selective in their mechanisms of action. SARMS have a special affinity for certain tissues like muscle and bone, but not for other tissues like the prostate, liver, and brain. They also don’t convert into unwanted molecules that cause side effects, like DHT and estrogen. This makes side effects associated with steroid usage like gynecomastia (gyno), water retention, hair loss etc. impossible with SARM usage.Some SARMS will suppress natural testosterone production and HPTA function but their rate of suppression is minimal, and a mini post cycle therapy (PCT) with a good natural testosterone booster is all that is needed after a cycle of SARMS.
