


drtbear1967
Musclechemistry Board Certified Member
Post Cycle Therapy
Introduction To Post Cycle Therapy
Post cycle therapy (PCT) is perhaps the most important aspect of anabolic steroid use. The concept of PCT did not exist prior to the late 1980s and early 1990s, as the understanding of the mechanisms by which anabolic steroids affected the body were not completely understood during the 1950s, 1960s, and 1970s. It was during this time period where doctors, scientists, and anabolic steroid users were only beginning to learn about the dynamics of anabolic steroids and how they affect the endocrine system. It was understood since the beginning of anabolic steroid use that the exogenous administration of anabolic steroids resulted in triggering the body’s negative feedback loop of the HPTA (Hypothalamic Pituitary Testicular Axis) and that endogenous Testosterone production would, as a result, become suppressed and/or shut down. Unfortunately during the early periods of anabolic steroid use (between the 1950s and 1990), there was limited access to any compounds or knowledge as to how to effectively mitigate this effect.
Today it is a very different story, where scientific and medical understanding of anabolic steroid use has soared exponentially since the old ‘golden era’ days of bodybuilding and anabolic steroid use in athletics. Countless developments of beneficial compounds for the purpose of hormonal recovery after anabolic steroid use, alongside the increased scientific and medical knowledge, has enabled anabolic steroid use and its associated endocrine disruptions to become a far safer endeavor than it ever once was. With the proper knowledge of how to properly and efficiently recover the body’s HPTA and hormonal systems through post cycle therapy (PCT), individuals can not only emerge from their anabolic steroid cycles while holding on to almost all of their muscle gains, but they can also increase the chances upwards of the 90% or higher range of emerging with a fully functional endocrine system and a healthy HPTA.
Following the use of exogenous anabolic steroids, the majority of users will experience what has been dubbed a “hormonal crash” or “post cycle crash”, which is a bodily environment in which key hormones essential to the retention of the newly created muscle mass has been suppressed or shut down. The key hormones in question are LH (Luteinizing Hormone), FSH (Follicle Stimulating Hormone), and subsequently (and most importantly), Testosterone. LH and FSH are known as gonadotropins, which are hormones that signal the gonads (testes) to begin or increase the manufacture and secretion of Testosterone. Alongside low levels of these hormones, the overall balance of total hormones will be essentially thrown off, whereby Testosterone levels will be low, and most of the time (depending on many factors), Estrogen levels will be higher, and levels of Cortisol (a steroid hormone that destroys muscle tissue) will be at normal levels. With Testosterone levels low and Cortisol levels in the normal (or high) range, Cortisol now becomes a threat to the newly created muscle that was created during the recent anabolic steroid cycle (Testosterone properly suppresses and counteracts Cortisol’s catabolic effects on muscle tissue). SHBG (Sex Hormone Binding Globulin) is also a concern here as well, which is a protein that binds to sex hormones (Testosterone) and renders them inactive, essentially ‘handcuffing’ them and preventing them from exerting their effects. SHBG will also normally be elevated during the post-cycle weeks as a result of the supraphysiological levels of androgens from the recent anabolic steroid cycle.
The human body will normally restore this imbalance of hormones and recover its endogenous Testosterone levels on its own over time with no assistance, but studies have demonstrated that without the intervention of Testosterone stimulating agents, this will occur over the course of 1 – 4 months. This is quite evidently enough time for the hormonal imbalance to wreak havoc on the body and result in any individual losing most or all of the newly gained muscle during this time. Therefore, all anabolic steroid users should be concerned with the fastest possible hormonal recovery, assisted and boosted with the use of Testosterone stimulating compounds in the proper manner. Furthermore, the attempt to allow the body to recover on its own will present a very high probability of long-term endocrine damage to the HPTA over time whereby the individual will develop anabolic steroid induced hypogonadism (the inability to manufacture proper levels of Testosterone for the rest of their life). It is therefore paramount that a proper post cycle therapy that includes multiple recovery compounds be utilized so as to not only restore the HPTA function to normal levels as quickly as possible, but to avoid any possible permanent damage, which takes priority over the concern of maintaining the recently gained muscle mass.
What Post Cycle Therapy Protocol To Use?
There exist many different types of PCT protocols that have been developed over the years, and upon first glance, any individual will become extremely confused at how many different opinions exist among the anabolic steroid using community, as well as how many different established PCT protocols there are in existence. This article will present forth the best possible and most efficient post cycle therapy protocol backed by valid scientific data and logical reasoning. This article will also dispel various myths in regards to PCT, and outline which PCT protocols should not be followed due to recent more advanced developments, as well as recent better scientific and medical understandings of how a proper post cycle therapy protocol should work. At this point in time, there still exists very obsolete – and subsequently ineffective – PCT protocols that are still utilized by many anabolic steroid users, and this presents a serious hazard not only for the individual unknowingly using an obsolete post cycle therapy program, but to any individuals that might be observing, learning, and gathering ideas from that individual.
Without the proper understanding of what is specifically occurring within the endocrine system during these crucial weeks, as well as a lack of understanding of which compounds to utilize, what each compound does, and how to properly utilize them, serious problems can result.
The HPTA: How It Works
The HPTA is the Hypothalamic Pituitary Testicular Axis, which is an axis of interconnected endocrine glands in the body that deal with and control Testosterone production.
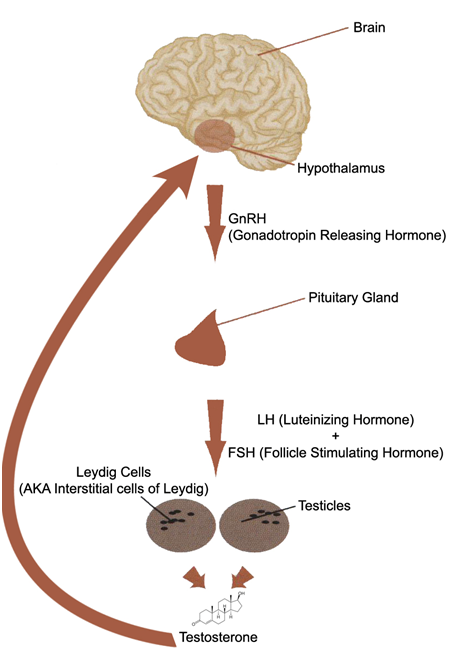
Outlined above is a diagram of the HPTA. The HPTA regulates how much Testosterone is manufactured and circulating the body at any one given time. Every individual is essentially programmed by their genetics (DNA) as to how much maximum Testosterone they will manufacture, and this is the prime determining factor. There exist other factors that determine how much Testosterone an individual will produce as well, and these include: age, diet, body composition, lifestyle habits, and physical activity. All of these factors play a role in how much Testosterone an individual will generate overall.
The HPTA functions under what is known as the negative feedback loop, whereby the body will reduce its manufacture and secretion of Testosterone if too much Testosterone is detected circulating in the body, and will also adjust as such if insufficient amounts of Testosterone are detected. This detection and adjustment, known as the negative feedback loop, is controlled by the hypothalamus, which is essentially considered the ‘master’ gland for all endocrine and hormonal functions in the body. The negative feedback loop is ultimately the body’s attempt to maintain hormonal homeostasis, which refers to the regulation of a system (in this case, the internal systems of the body) in order to maintain stable and constant favorable conditions. All endocrine glands operate by way of the negative feedback loop in one way or another, and to varying degrees. In the case of post cycle therapy, the concern is primarily with the negative feedback loop of the HPTA.
Within the HPTA, the concern during PCT is the restoration and regulation of the following 5 hormones to homeostasis:
– GnRH (Gonadotropin Releasing Hormone)
– LH (Luteinizing Hormone)
– FSH (Follicle Stimulating Hormone)
– Testosterone
The HPTA begins with the first axis point, the hypothalamus, which will detect a need for the human body to manufacture more Testosterone, and will release varying amounts of GnRH. GnRH is a hormone that signals the next axis point, the pituitary gland, to begin the manufacture and release of two important gonadotropins: LH and FSH. LH and FSH are two hormones that work to signal the third axis point, the testes, to begin production and secretion of Testosterone. This is the final stage of Testosterone production in the HPTA.
There are two primary hormonal factors that serve to inhibit, reduce, suppress, or shut down Testosterone production in the HPTA:
– Excess Testosterone
– Excess Estrogen
Although there exist other hormones that serve to inhibit and suppress HPTA function (such as Progestins and Prolactin), these are the two primary conditional hormones that are of concern. When the hypothalamus detects excess levels of Testosterone and/or Estrogen in the body (either from the use of exogenous androgens on an anabolic steroid cycle or otherwise), the hypothalamus will act to attempt to restore a balance by essentially doing the opposite of what was previously described. The hypothalamus will reduce or stop its production of GnRH, which halts production of LH and FSH, which ultimately reduces or halts production of Testosterone. Until the hypothalamus’ ideal hormonal environment is restored, the production of the various signaling hormones within the HPTA will not begin, and this will often require months of time for the body to do this on its own without the intervention of any Testosterone stimulating agents. The reason as to why the recovery of the HPTA naturally takes such a long time should be very clear due to the described workings of the HPTA.
This very basic understanding of the mechanisms of the HPTA and negative feedback loop described above is essential to understanding how and why a proper PCT program must be developed and utilized following an anabolic steroid cycle.
Determining Factors In Difficulty Recovering the HPTA
With anabolic steroid use, there are several different major determining factors in how much difficulty an individual will experience in recovery of their HPTA and endogenous Testosterone function during PCT. They are the following factors, in no particular order of importance:
1. Individual response
2. Type of anabolic steroid(s) used
3. Length of cycle (degree of testicular desensitization)
1. Individual response: Every single individual will respond in a different manner to any chemical, compound, anabolic steroid, food or drug in existence. While some individuals might experience absolutely no HPTA suppression or shutdown at all, other individuals might experience severe HPTA suppression and shutdown to the extent where they might require far longer periods of time to ensure full recovery than most. This, like anything else, is a spectrum whereby there are the very ‘lucky’ individuals that recover very quickly and easily on one end of the spectrum, and the ‘unlucky’ individuals that have extreme difficulty recovering during post cycle therapy. In between the two extremes is the average. Once again, this is due to the individual’s genetic programming as to how the HPTA will respond and attempt to maintain homeostasis.
2. Type of anabolic steroid(s) used: All anabolic steroids exhibit suppression or shutdown of the HPTA through the mechanisms of the negative feedback loop, and there are no exceptions to this. Various anabolic steroids are known as being mildly suppressive, while others are known as being heavily suppressive. This is all reliant on various different reasons, many of which will not be discussed here. In any case, no matter how mild or severe an anabolic steroid exerts HPTA suppression, all anabolic steroids when utilized for typical cycle lengths of weeks at a time will eventually cause the HPTA to shut down, or at the very least severely suppress its hormonal signal processes.
3. Length of cycle (degree of testicular desensitization): This is perhaps the most important and most influential factor. As the length of anabolic steroid use continues, the majority of the Leydig cells of the testes remain dormant and inactive, and the longer these interstitial cells remain dormant and inactive, the greater the difficulty in essentially getting these cells to respond to the stimulus of LH and FSH once again. It has been discovered in studies that the issue of recovery of the Leydig cells following anabolic steroid use is not due to a lack of LH, but due instead to the desensitization of the Leydig cells to LH[1]. In one study in which exogenous Testosterone was administered to male test subjects for 21 weeks, LH levels were suppressed shortly after beginning administration. However, at the end of the 21 week period, LH levels were observed to rise within 3 weeks once the exogenous Testosterone administration stopped, but Testosterone levels did not rise until many weeks later in most of the test subjects.
The Three Primary Testosterone Stimulating Agents for HPTA Recovery During PCT
Before delving into the three different types of Testosterone stimulating compounds for hormonal recovery during post cycle therapy, it is very important for individuals to understand that the use of any one single compound except for a single select one or two is inadequate for hormonal recovery during PCT. Ideally, all post cycle therapy programs should be a multi-component PCT program that includes several different compounds that work in tandem with one another in order to provide the most effective and fastest possible HPTA recovery following an anabolic steroid cycle.
The three categories of compounds are (in order of importance):
1. SERMs (Selective Estrogen Receptor Modulators)
2. Aromatase Inhibitors
3. HCG( Human Chorionic Gonadotropin)
SERMs: Classes of drugs in the SERM category include: Nolvadex (Tamoxifen Citrate), Clomid (Clomiphene Citrate), Raloxifene, and Fareston (Toremifene Citrate). The nature of a SERM is that it exhibits mixed Estrogen agonist and Estrogen antagonist effects on the body. This means that although a SERM might block the effect of Estrogen at the cellular level in certain tissues, it can enhance Estrogenic effects in other areas of the body. These can be positive effects as well as negative effects. Nolvadex, for example, exhibits Estrogenic agonistic effects in the liver, which for all intents and purposes is a positive effect, as its effects here result in a positive change in cholesterol profiles (something desired by many). All SERMs to varying degrees serve to act as an Estrogen antagonist in this area, acting to mitigate Estrogen’s effects on breast tissue, reducing or blocking the side effect of gynecomastia. In terms of the effect of SERMs on endogenous Testosterone stimulation, they serve to act as an Estrogen antagonist at the pituitary gland, triggering the release of LH and FSH as a result. Elevated levels of Estrogen in men can and does suppress the output of endogenous Testosterone via the negative feedback loop, leading to hypogonadism[2]. SERMs for this purpose are an absolutely essential addition to any PCT protocol and are not to be excluded under any circumstance. Regardless of this, however, the sole focus should not be on SERMs.
Aromatase inhibitors: These are compounds such as Aromasin (Exemestane), Arimidex (Anastrozole), and Letrozole (Femara). Rather than block the activity of Estrogen at the cellular level in different tissues, aromatase inhibitors (AIs) serve to lower total circulating Estrogen levels in the body by way of inhibiting the aromatase enzyme, which is the enzyme responsible for the conversion of androgens into Estrogen. The conversion of androgens into Estrogen results in excess Estrogen levels, which, as explained earlier in this article, will trigger the negative feedback loop leading to suppression of Testosterone production. By way of lowering total circulating blood plasma Estrogen levels, AIs will engage the negative feedback loop in a positive manner and result in the release of LH and FSH for the manufacture and secretion of more Testosterone. This is essentially due to the hypothalamus realizing that circulating Estrogen levels are too low, and will attempt to increase circulating levels of Testosterone in order for a portion of the Testosterone secreted to be able to become aromatized into Estrogen in order to restore the hormonal balance. The other importance of aromatase inhibitors is the ability to mitigate the Estrogenic effects of HCG, which will be explained shortly. It is important to note, however, that the majority of aromatase inhibitors do not comply very well with SERMs such as Nolvadex, and that very specific choices should be made in regards as to which AI is used during PCT.
HCG: Human Chorionic Gonadotropin is, for the most part, synthetic LH. It is a protein hormone manufactured in high amounts by pregnant females that contains a protein subunit that is 100% identical to LH, and therefore when administered to men, it will mimic the action of LH in target tissues, such as the testes. What results is an increase in Testosterone production via stimulation of the Leydig cells by HCG. HCG should never be utilized alone, as its nature as a gonadotropin will itself trigger a negative feedback loop whereby once HCG is utilized, the pituitary gland will halt output of LH until HCG use has discontinued. Therefore, HCG must be utilized with a SERM and especially an aromatase inhibitor, as HCG has demonstrated to increase aromatase activity in the testes, resulting in rising Estrogen levels[3].
Putting Them All Together
The reader may be wondering which compounds to select of the three categories listed, and how to properly use them. The answer lies in understanding the properties of each and, in understanding these properties, how to use them efficiently and appropriately.
HCG
The first item to be examined will be HCG. The majority of anabolic steroid users from the 1960s – mid 1980s did not even utilize any compounds for the purpose of hormonal recovery, and the term PCT did not even exist at that time. When the use of HCG became increasingly popular (circa 1980), it was the only compound utilized. Since then, the medical and scientific understanding of such things has increased exponentially and there should be no reason for any informed and properly educated individual to utilize HCG on its own for PCT. When utilized in conjunction with one of the other two categories of compounds (an AI and a SERM), the dynamics change considerably.
It has been mentioned already that much of the difficulty in recovering the HPTA following an anabolic steroid cycle is the result of Leydig cell desensitization. HCG is essentially an analogue of LH, and the testes after a prolonged anabolic steroid cycle would be as equally desensitized to HCG as they are to LH. The human body, however, produces LH amounts on its own that are far too inefficient for proper and rapid Testosterone production. The body’s natural increase of LH and FSH following an anabolic steroid cycle is also not a rapid peak, but a very slow and steady incline, as evidenced by the study referenced earlier in which it was not until 3 weeks when LH levels only began to reach the normal physiological measurements following the cessation of exogenous Testosterone. Therefore, the body’s own natural LH production does not provide a high enough dose for stimulation, nor an immediate stimulation to the testes required for the initial increase in Testosterone needed during the post cycle therapy weeks.
HCG, utilized in a specific manner during the first 1 – 2 weeks of PCT at a dose of 100-1,500IU every 2 days, is what allows the individual to provide the testes with a high dose to provide them with a ‘shock’ effect, and sustain this shock effect on the Leydig cells of the testes for a sustained period of the first 1 – 2 weeks of post cycle therapy. Studies have in fact demonstrated the incredible effectiveness of HCG for this purpose, and it is even suggested clinically that HCG be utilized for the purpose of treating anabolic steroid induced hypogonadism[4]. Following this line of thought, the other two compounds (the SERM and the AI) are to be utilized as supportive compounds for HCG use in this 1 – 2 week period, and after HCG is discontinued early on in PCT, only the SERM is to be used in order to carry along the hormonal recovery process.
In spite of the good news in regards to the ability for HCG to assist in hormonal recovery, there are still two remaining issues to be addressed:
– The fact that HCG causes increased production of aromatase, leading to increased Estrogen levels.
– Following the discontinuation of HCG, the body is left with very little endogenous LH and FSH production due to the exogenous administration of HCG.
Aromatase Inhibitors: Aromasin (Exemestane) Above All Else
The first of the two remaining issues to be addressed will be the fact that HCG will trigger increases in testicular aromatase expression, and result in Estrogen increases in the body. It should also be noted that it will cause an increase in testicular progesterone levels. Estrogen rising is of course undesirable during PCT, as it has already been explained that Estrogen will trigger suppression of endogenous Testosterone production, and there is no doubt that any individual wishes to encounter Estrogenic side effects during PCT either.
Therefore, the option here is to include an aromatase inhibitor. However, there exists a big problem in regards to the other two of the three major aromatase inhibitors (Arimidex and Letrozole). The issue is the fact that in a PCT program that includes the use of SERMs such as Nolvadex and Clomid, which are known as absolutely essential components to a PCT program, Arimidex and Letrozole have direct negative interactions with Nolvadex. The problem here is that Arimidex (or Letrozole) and Nolvadex both directly counteract one another. One study has demonstrated that when Arimidex is utilized with Nolvadex, Nolvadex will decrease blood plasma concentration of Arimidex (as well as Letrozole, another commonly used aromatase inhibitor)[5]. The conclusion here is that the use of Arimidex or Letrozole with Nolvadex together is a very bad idea and may work counterproductively if used together in a PCT protocol. Aromasin completely circumvents this problem, as it has been demonstrated to have no interactions what so ever with Nolvadex, unlike the other two aforementioned aromatase inhibitors. In one study, Aromasin displayed no such reduced effectiveness or any reduced blood plasma levels when utilized with Nolvadex[6].
The other benefit of selecting Aromasin over all other AIs is the fact that Aromasin has demonstrated in several studies to impact cholesterol profiles in a negative manner far less than other aromatase inhibitors have, where in one particular study on cancer patients, 24 weeks of Aromasin (Exemestane) administration held no impact on cholesterol profiles[7]. Some other studies have also demonstrated a nil effect on cholesterol profiles from the use of Aromasin[8]. Although there have also been some studies that have demonstrated a negative effect on cholesterol profiles resultant from Aromasin use, it is evident that there is not as a significant or as a negatively impacting effect from Aromasin on cholesterol as other aromatase inhibitors[9].
Finally, in addition to these benefits from Aromasin, it is very clear that Aromasin holds the ability to increase Testosterone levels in males as demonstrated by studies. For example, one particularly notable study selected 12 healthy young male test subjects, and were administered random Aromasin doses of 25mg and 50mg for a 10 day period, and not only was Estrogen suppressed by a significant amount (38%), but Testosterone levels in the test subjects were observed to have increased by an incredible 60%[10].
Following these details, Aromasin would be the best possible aromatase inhibitor of choice in order to combat the increased aromatase activity caused by HCG. Therefore, Aromasin would then be utilized at a full 25mg daily dose, and only while HCG is utilized. Once HCG is discontinued, Aromasin too should be halted.
The only following issue to cover now is that of stimulating and maintaining proper endogenous LH release so as to carry recovery along until the body can become self-sufficient once again.
ERMs: Nolvadex and Clomid
The question is often asked among the anabolic steroid using community: Clomid or Nolvadex? Which one for PCT?
First of all, the best possible addition to HCG in a PCT protocol is Nolvadex (Tamoxifen Citrate), as studies have demonstrated that HCG and Nolvadex utilized together have exhibited a remarkable synergistic effect in terms of stimulating endogenous Testosterone production, and that Nolvadex will actually work to block the desensitization effect on the Leydig cells of the testes caused by high doses of HCG[11]. This is very important, because just as too little LH secretion for extended periods can cause desensitization to gonadotropins, too much gonadotropin stimulation (in the form of HCG or otherwise) will likewise cause a desensitization effect.
Secondly, Nolvadex on a mg for mg basis is far more effective than Clomid in stimulating endogenous Testosterone production, as well as being a more cost-effective choice than Clomid itself. Studies have demonstrated that 150mg of Clomid (Clomiphene Citrate) administered daily raised endogenous Testosterone levels of 10 healthy males by approximately 150%, while incidentally, 20mg of Nolvadex (Tamoxifen Citrate) daily raised endogenous Testosterone levels by the same amount[12]. It is very evident here that Clomid is very effective for this purpose, but Nolvadex seems to be a more cost-effective choice seeing as though it is more effective than Clomid when compared mg for mg. The benefits of Nolvadex over Clomid do not end there – Clomid, although it does exhibit Estrogen antagonist effects at the pituitary gland like Nolvadex does, actually exhibits Estrogen agonist effects there too[13]. What this means is that Clomid will actually work in varying degrees as an Estrogen at the pituitary gland, triggering the negative feedback loop and reducing the output of Testosterone stimulating gonadotropins (LH and FSH). This is a very serious problem during post cycle therapy, which is a period in which individuals are trying to recover their HPTA function rather than halt it even further. Ideally, one would want a SERM that exhibits almost 100% Estrogen antagonistic effects on the pituitary gland, and Nolvadex is the perfect choice for this.
When it comes to the dosing aspect of Nolvadex, The standard dose for PCT and for stimulating the release of GnRH (Gonadotropin Releasing Hormone), LH, FSH, and ultimately Testosterone is that of a simple Nolvadex dose of 20 – 40mg daily. In all studies involving Nolvadex doses used to stimulate endogenous Testosterone production, only 20 – 40mg daily of Nolvadex was utilized, and it has in fact been shown that doubling the dose to 40mg or any higher will not produce any significant difference in endogenous Testosterone secretion. The only reason why many elect to utilize 40mg daily of Nolvadex for the first 1-2 weeks of a PCT program is for the purpose of achieving optimal peak blood plasma levels quicker so as to ensure HPTA recovery quicker.
T
he Final Layout
The ideal post cycle therapy protocol should then be as follows:
4 – 6 weeks Total PCT time (depending on recovery ability of the individual)
Weeks 1 – 2:
– HCG at 1000iu/E2D
– Aromasin (Exemestane) at 25mg/day
– Nolvadex (Tamoxifen Citrate) at 40mg/day
Weeks 2 – 6:
– Nolvadex (Tamoxifen Citrate) at 20mg/day
Additional Optional Components (Vitamins/Supplements/Compounds) to Aid During PCT
Aside from the main components discussed, there are various other components that are largely optional, but still very effective for hormonal recovery of the HPTA during the post cycle therapy weeks.
Vitamin D (Cholecalciferol): There is plenty of established solid evidence through studies that mega dosing Vitamin D (Cholecalciferol) exhibits a significant effect on increasing Testosterone levels in men and also has a significant ability to suppress SHBG levels in the body. One of the best PCT additions is indeed Vitamin D. There is an overabundance of clinical studies in existence demonstrating that low Vitamin D levels corresponds with a low level of endogenous Testosterone production (particularly in the winter months for obvious reasons). In one study conducted in Austria where about 200 subjects were involved with one group administered 3332iu daily of vitamin D, and a placebo group, results had shown that men with sufficient Vitamin D levels had significantly higher levels of Testosterone and significantly lower levels of SHBG when compared to the D-deficient subjects[14]. Androgen levels and Vitamin D levels are associated in men and reveal a concordant seasonal variation[15]. In various other studies, similar findings were reported where subjects who were administered higher amounts of Vitamin D over time demonstrated vast increases in total Testosterone levels, and decreases in SHBG. Anecdotal evidence of people who have been supplementing with vitamin D and getting regular blood work at their doctors are observing large increases in their total and free testosterone levels approximately 1 – 2 months after supplementing with Vitamin D.
Medical References:
[1] Effect of long-term testosterone enanthate administration on male reproductive function: Clinical evaluation, serum FSH, LH, Testosterone and seminal fluid analysis in normal men. J. Mauss, G. Borsch et al. Acta Endocrinol 78 (1975) 373-84.
[2] “Dangers of Excess Estrogen In the Aging Male”. Faloon, William. Life Extension Magazine, November 2008.
[3] Acute stimulation of aromatization in Leydig cells by human chorionic gonadotropin in vitro. Proc Natl Acad Sci USA 76:4460-3/1979.
[4] Anabolic steroid induced hypogonadism treated with human chorionic gonadotropin. Gill GV. Postgrad Med J. 1998 Jan;74(867):45-6.
[5] Comparative clinical pharmacology and pharmacokinetic interactions of aromatase inhibitors. Boeddinghaus IM, Dowsett M. J Steroid Biochem Mol Biol. 2001 Dec;79(1-5):85-91.
[6] Inhibitory effect of combined treatment with the aromatase inhibitor exemestane and tamoxifen on DMBA-induced mammary tumors in rats. Zaccheo T, Giudici D, Di Salle E. J Steroid Biochem Mol Biol. 1993 Mar;44(4-6):677-80.
[7] No adverse impact on serum lipids of the irreversible aromatase inactivator Aromasin [Exemestane (E)] in first-line treatment of metastatic breast cancer (MBC): companion study to a European Organization of Research and Treatment of Cancer (Breast Group) Trial with Pharmacia Upjohn. Lohrisch C., Paridaens R., Dirix L. Y., Beex M., Nooij M., Cameron D. Proc. Am. Soc. Clin. Oncol., 20: 43a 2001.
[8] Pharmacokinetics and dose finding of a potent aromatase inhibitor, aromasin (exemestane), in young males. Mauras N, Lima J, Patel D, Rini A, di Salle E, Kwok A, Lippe B. J Clin Endocrinol Metab. 2003 Dec;88(12):5951-6.
[9] Plasma changes in breast cancer patients during endocrine therapy: lipid measurements and nuclear magnetic resonance (NMR) spectroscopy. Engan T., Krane J., Johannessen D. C., Kvinnsland S. Breast Cancer Res. Treat., 36: 287-297, 1995.
[10] Pharmacokinetics and dose finding of a potent aromatase inhibitor, aromasin (exemestane), in young males. Mauras N, Lima J, Patel D, Rini A, di Salle E, Kwok A, Lippe B. J Clin Endocrinol Metab. 2003 Dec;88(12):5951-6.
[11] Tamoxifen suppresses gonadotropin-induced 17 alpha-hydroxyprogesterone accumulation in normal men. Smals AG, Pieters GF, Drayer JI, Boers GH, Benraad TJ, Kloppenborg PW. J Clin Endocrinol Metab. 1980 Nov;51(5):1026-9.
[12] Hormonal effects of an antiestrogen, tamoxifen, in normal and oligospermic men. Vermeulen A, Comhaire F. Fertil Steril. 1978 Mar;29(3):320-7.
[13] Disparate effect of clomiphene and tamoxifen on pituitary gonadotropin release in vitro. Adashi EY, Hsueh AJ, Bambino TH, Yen SS. Am J Physiol 1981 Feb;240(2):E125-30
[14] Effect of vitamin D supplementation on testosterone levels in men. Pilz S, Frisch S, Koertke H, Kuhn J, Dreier J, Obermayer-Pietsch B, Wehr E, Zittermann A. Horm Metab Res. 2011 Mar;43(3):223-5. doi: 10.1055/s-0030-1269854. Epub 2010 Dec 10.
[15] Association of vitamin D status with serum androgen levels in men. Wehr E, Pilz S, Boehm BO, März W, Obermayer-Pietsch B. Department of Internal Medicine, Division of Endocrinology and Nuclear Medicine, Medical University Graz, Graz, Austria. 2010 Aug;73(2):243-8
Introduction To Post Cycle Therapy
Post cycle therapy (PCT) is perhaps the most important aspect of anabolic steroid use. The concept of PCT did not exist prior to the late 1980s and early 1990s, as the understanding of the mechanisms by which anabolic steroids affected the body were not completely understood during the 1950s, 1960s, and 1970s. It was during this time period where doctors, scientists, and anabolic steroid users were only beginning to learn about the dynamics of anabolic steroids and how they affect the endocrine system. It was understood since the beginning of anabolic steroid use that the exogenous administration of anabolic steroids resulted in triggering the body’s negative feedback loop of the HPTA (Hypothalamic Pituitary Testicular Axis) and that endogenous Testosterone production would, as a result, become suppressed and/or shut down. Unfortunately during the early periods of anabolic steroid use (between the 1950s and 1990), there was limited access to any compounds or knowledge as to how to effectively mitigate this effect.
Today it is a very different story, where scientific and medical understanding of anabolic steroid use has soared exponentially since the old ‘golden era’ days of bodybuilding and anabolic steroid use in athletics. Countless developments of beneficial compounds for the purpose of hormonal recovery after anabolic steroid use, alongside the increased scientific and medical knowledge, has enabled anabolic steroid use and its associated endocrine disruptions to become a far safer endeavor than it ever once was. With the proper knowledge of how to properly and efficiently recover the body’s HPTA and hormonal systems through post cycle therapy (PCT), individuals can not only emerge from their anabolic steroid cycles while holding on to almost all of their muscle gains, but they can also increase the chances upwards of the 90% or higher range of emerging with a fully functional endocrine system and a healthy HPTA.
Following the use of exogenous anabolic steroids, the majority of users will experience what has been dubbed a “hormonal crash” or “post cycle crash”, which is a bodily environment in which key hormones essential to the retention of the newly created muscle mass has been suppressed or shut down. The key hormones in question are LH (Luteinizing Hormone), FSH (Follicle Stimulating Hormone), and subsequently (and most importantly), Testosterone. LH and FSH are known as gonadotropins, which are hormones that signal the gonads (testes) to begin or increase the manufacture and secretion of Testosterone. Alongside low levels of these hormones, the overall balance of total hormones will be essentially thrown off, whereby Testosterone levels will be low, and most of the time (depending on many factors), Estrogen levels will be higher, and levels of Cortisol (a steroid hormone that destroys muscle tissue) will be at normal levels. With Testosterone levels low and Cortisol levels in the normal (or high) range, Cortisol now becomes a threat to the newly created muscle that was created during the recent anabolic steroid cycle (Testosterone properly suppresses and counteracts Cortisol’s catabolic effects on muscle tissue). SHBG (Sex Hormone Binding Globulin) is also a concern here as well, which is a protein that binds to sex hormones (Testosterone) and renders them inactive, essentially ‘handcuffing’ them and preventing them from exerting their effects. SHBG will also normally be elevated during the post-cycle weeks as a result of the supraphysiological levels of androgens from the recent anabolic steroid cycle.
The human body will normally restore this imbalance of hormones and recover its endogenous Testosterone levels on its own over time with no assistance, but studies have demonstrated that without the intervention of Testosterone stimulating agents, this will occur over the course of 1 – 4 months. This is quite evidently enough time for the hormonal imbalance to wreak havoc on the body and result in any individual losing most or all of the newly gained muscle during this time. Therefore, all anabolic steroid users should be concerned with the fastest possible hormonal recovery, assisted and boosted with the use of Testosterone stimulating compounds in the proper manner. Furthermore, the attempt to allow the body to recover on its own will present a very high probability of long-term endocrine damage to the HPTA over time whereby the individual will develop anabolic steroid induced hypogonadism (the inability to manufacture proper levels of Testosterone for the rest of their life). It is therefore paramount that a proper post cycle therapy that includes multiple recovery compounds be utilized so as to not only restore the HPTA function to normal levels as quickly as possible, but to avoid any possible permanent damage, which takes priority over the concern of maintaining the recently gained muscle mass.
What Post Cycle Therapy Protocol To Use?
There exist many different types of PCT protocols that have been developed over the years, and upon first glance, any individual will become extremely confused at how many different opinions exist among the anabolic steroid using community, as well as how many different established PCT protocols there are in existence. This article will present forth the best possible and most efficient post cycle therapy protocol backed by valid scientific data and logical reasoning. This article will also dispel various myths in regards to PCT, and outline which PCT protocols should not be followed due to recent more advanced developments, as well as recent better scientific and medical understandings of how a proper post cycle therapy protocol should work. At this point in time, there still exists very obsolete – and subsequently ineffective – PCT protocols that are still utilized by many anabolic steroid users, and this presents a serious hazard not only for the individual unknowingly using an obsolete post cycle therapy program, but to any individuals that might be observing, learning, and gathering ideas from that individual.
Without the proper understanding of what is specifically occurring within the endocrine system during these crucial weeks, as well as a lack of understanding of which compounds to utilize, what each compound does, and how to properly utilize them, serious problems can result.
The HPTA: How It Works
The HPTA is the Hypothalamic Pituitary Testicular Axis, which is an axis of interconnected endocrine glands in the body that deal with and control Testosterone production.
Outlined above is a diagram of the HPTA. The HPTA regulates how much Testosterone is manufactured and circulating the body at any one given time. Every individual is essentially programmed by their genetics (DNA) as to how much maximum Testosterone they will manufacture, and this is the prime determining factor. There exist other factors that determine how much Testosterone an individual will produce as well, and these include: age, diet, body composition, lifestyle habits, and physical activity. All of these factors play a role in how much Testosterone an individual will generate overall.
The HPTA functions under what is known as the negative feedback loop, whereby the body will reduce its manufacture and secretion of Testosterone if too much Testosterone is detected circulating in the body, and will also adjust as such if insufficient amounts of Testosterone are detected. This detection and adjustment, known as the negative feedback loop, is controlled by the hypothalamus, which is essentially considered the ‘master’ gland for all endocrine and hormonal functions in the body. The negative feedback loop is ultimately the body’s attempt to maintain hormonal homeostasis, which refers to the regulation of a system (in this case, the internal systems of the body) in order to maintain stable and constant favorable conditions. All endocrine glands operate by way of the negative feedback loop in one way or another, and to varying degrees. In the case of post cycle therapy, the concern is primarily with the negative feedback loop of the HPTA.
Within the HPTA, the concern during PCT is the restoration and regulation of the following 5 hormones to homeostasis:
– GnRH (Gonadotropin Releasing Hormone)
– LH (Luteinizing Hormone)
– FSH (Follicle Stimulating Hormone)
– Testosterone
The HPTA begins with the first axis point, the hypothalamus, which will detect a need for the human body to manufacture more Testosterone, and will release varying amounts of GnRH. GnRH is a hormone that signals the next axis point, the pituitary gland, to begin the manufacture and release of two important gonadotropins: LH and FSH. LH and FSH are two hormones that work to signal the third axis point, the testes, to begin production and secretion of Testosterone. This is the final stage of Testosterone production in the HPTA.
There are two primary hormonal factors that serve to inhibit, reduce, suppress, or shut down Testosterone production in the HPTA:
– Excess Testosterone
– Excess Estrogen
Although there exist other hormones that serve to inhibit and suppress HPTA function (such as Progestins and Prolactin), these are the two primary conditional hormones that are of concern. When the hypothalamus detects excess levels of Testosterone and/or Estrogen in the body (either from the use of exogenous androgens on an anabolic steroid cycle or otherwise), the hypothalamus will act to attempt to restore a balance by essentially doing the opposite of what was previously described. The hypothalamus will reduce or stop its production of GnRH, which halts production of LH and FSH, which ultimately reduces or halts production of Testosterone. Until the hypothalamus’ ideal hormonal environment is restored, the production of the various signaling hormones within the HPTA will not begin, and this will often require months of time for the body to do this on its own without the intervention of any Testosterone stimulating agents. The reason as to why the recovery of the HPTA naturally takes such a long time should be very clear due to the described workings of the HPTA.
This very basic understanding of the mechanisms of the HPTA and negative feedback loop described above is essential to understanding how and why a proper PCT program must be developed and utilized following an anabolic steroid cycle.
Determining Factors In Difficulty Recovering the HPTA
With anabolic steroid use, there are several different major determining factors in how much difficulty an individual will experience in recovery of their HPTA and endogenous Testosterone function during PCT. They are the following factors, in no particular order of importance:
1. Individual response
2. Type of anabolic steroid(s) used
3. Length of cycle (degree of testicular desensitization)
1. Individual response: Every single individual will respond in a different manner to any chemical, compound, anabolic steroid, food or drug in existence. While some individuals might experience absolutely no HPTA suppression or shutdown at all, other individuals might experience severe HPTA suppression and shutdown to the extent where they might require far longer periods of time to ensure full recovery than most. This, like anything else, is a spectrum whereby there are the very ‘lucky’ individuals that recover very quickly and easily on one end of the spectrum, and the ‘unlucky’ individuals that have extreme difficulty recovering during post cycle therapy. In between the two extremes is the average. Once again, this is due to the individual’s genetic programming as to how the HPTA will respond and attempt to maintain homeostasis.
2. Type of anabolic steroid(s) used: All anabolic steroids exhibit suppression or shutdown of the HPTA through the mechanisms of the negative feedback loop, and there are no exceptions to this. Various anabolic steroids are known as being mildly suppressive, while others are known as being heavily suppressive. This is all reliant on various different reasons, many of which will not be discussed here. In any case, no matter how mild or severe an anabolic steroid exerts HPTA suppression, all anabolic steroids when utilized for typical cycle lengths of weeks at a time will eventually cause the HPTA to shut down, or at the very least severely suppress its hormonal signal processes.
3. Length of cycle (degree of testicular desensitization): This is perhaps the most important and most influential factor. As the length of anabolic steroid use continues, the majority of the Leydig cells of the testes remain dormant and inactive, and the longer these interstitial cells remain dormant and inactive, the greater the difficulty in essentially getting these cells to respond to the stimulus of LH and FSH once again. It has been discovered in studies that the issue of recovery of the Leydig cells following anabolic steroid use is not due to a lack of LH, but due instead to the desensitization of the Leydig cells to LH[1]. In one study in which exogenous Testosterone was administered to male test subjects for 21 weeks, LH levels were suppressed shortly after beginning administration. However, at the end of the 21 week period, LH levels were observed to rise within 3 weeks once the exogenous Testosterone administration stopped, but Testosterone levels did not rise until many weeks later in most of the test subjects.
The Three Primary Testosterone Stimulating Agents for HPTA Recovery During PCT
Before delving into the three different types of Testosterone stimulating compounds for hormonal recovery during post cycle therapy, it is very important for individuals to understand that the use of any one single compound except for a single select one or two is inadequate for hormonal recovery during PCT. Ideally, all post cycle therapy programs should be a multi-component PCT program that includes several different compounds that work in tandem with one another in order to provide the most effective and fastest possible HPTA recovery following an anabolic steroid cycle.
The three categories of compounds are (in order of importance):
1. SERMs (Selective Estrogen Receptor Modulators)
2. Aromatase Inhibitors
3. HCG( Human Chorionic Gonadotropin)
SERMs: Classes of drugs in the SERM category include: Nolvadex (Tamoxifen Citrate), Clomid (Clomiphene Citrate), Raloxifene, and Fareston (Toremifene Citrate). The nature of a SERM is that it exhibits mixed Estrogen agonist and Estrogen antagonist effects on the body. This means that although a SERM might block the effect of Estrogen at the cellular level in certain tissues, it can enhance Estrogenic effects in other areas of the body. These can be positive effects as well as negative effects. Nolvadex, for example, exhibits Estrogenic agonistic effects in the liver, which for all intents and purposes is a positive effect, as its effects here result in a positive change in cholesterol profiles (something desired by many). All SERMs to varying degrees serve to act as an Estrogen antagonist in this area, acting to mitigate Estrogen’s effects on breast tissue, reducing or blocking the side effect of gynecomastia. In terms of the effect of SERMs on endogenous Testosterone stimulation, they serve to act as an Estrogen antagonist at the pituitary gland, triggering the release of LH and FSH as a result. Elevated levels of Estrogen in men can and does suppress the output of endogenous Testosterone via the negative feedback loop, leading to hypogonadism[2]. SERMs for this purpose are an absolutely essential addition to any PCT protocol and are not to be excluded under any circumstance. Regardless of this, however, the sole focus should not be on SERMs.
Aromatase inhibitors: These are compounds such as Aromasin (Exemestane), Arimidex (Anastrozole), and Letrozole (Femara). Rather than block the activity of Estrogen at the cellular level in different tissues, aromatase inhibitors (AIs) serve to lower total circulating Estrogen levels in the body by way of inhibiting the aromatase enzyme, which is the enzyme responsible for the conversion of androgens into Estrogen. The conversion of androgens into Estrogen results in excess Estrogen levels, which, as explained earlier in this article, will trigger the negative feedback loop leading to suppression of Testosterone production. By way of lowering total circulating blood plasma Estrogen levels, AIs will engage the negative feedback loop in a positive manner and result in the release of LH and FSH for the manufacture and secretion of more Testosterone. This is essentially due to the hypothalamus realizing that circulating Estrogen levels are too low, and will attempt to increase circulating levels of Testosterone in order for a portion of the Testosterone secreted to be able to become aromatized into Estrogen in order to restore the hormonal balance. The other importance of aromatase inhibitors is the ability to mitigate the Estrogenic effects of HCG, which will be explained shortly. It is important to note, however, that the majority of aromatase inhibitors do not comply very well with SERMs such as Nolvadex, and that very specific choices should be made in regards as to which AI is used during PCT.
HCG: Human Chorionic Gonadotropin is, for the most part, synthetic LH. It is a protein hormone manufactured in high amounts by pregnant females that contains a protein subunit that is 100% identical to LH, and therefore when administered to men, it will mimic the action of LH in target tissues, such as the testes. What results is an increase in Testosterone production via stimulation of the Leydig cells by HCG. HCG should never be utilized alone, as its nature as a gonadotropin will itself trigger a negative feedback loop whereby once HCG is utilized, the pituitary gland will halt output of LH until HCG use has discontinued. Therefore, HCG must be utilized with a SERM and especially an aromatase inhibitor, as HCG has demonstrated to increase aromatase activity in the testes, resulting in rising Estrogen levels[3].
Putting Them All Together
The reader may be wondering which compounds to select of the three categories listed, and how to properly use them. The answer lies in understanding the properties of each and, in understanding these properties, how to use them efficiently and appropriately.
HCG
The first item to be examined will be HCG. The majority of anabolic steroid users from the 1960s – mid 1980s did not even utilize any compounds for the purpose of hormonal recovery, and the term PCT did not even exist at that time. When the use of HCG became increasingly popular (circa 1980), it was the only compound utilized. Since then, the medical and scientific understanding of such things has increased exponentially and there should be no reason for any informed and properly educated individual to utilize HCG on its own for PCT. When utilized in conjunction with one of the other two categories of compounds (an AI and a SERM), the dynamics change considerably.
It has been mentioned already that much of the difficulty in recovering the HPTA following an anabolic steroid cycle is the result of Leydig cell desensitization. HCG is essentially an analogue of LH, and the testes after a prolonged anabolic steroid cycle would be as equally desensitized to HCG as they are to LH. The human body, however, produces LH amounts on its own that are far too inefficient for proper and rapid Testosterone production. The body’s natural increase of LH and FSH following an anabolic steroid cycle is also not a rapid peak, but a very slow and steady incline, as evidenced by the study referenced earlier in which it was not until 3 weeks when LH levels only began to reach the normal physiological measurements following the cessation of exogenous Testosterone. Therefore, the body’s own natural LH production does not provide a high enough dose for stimulation, nor an immediate stimulation to the testes required for the initial increase in Testosterone needed during the post cycle therapy weeks.
HCG, utilized in a specific manner during the first 1 – 2 weeks of PCT at a dose of 100-1,500IU every 2 days, is what allows the individual to provide the testes with a high dose to provide them with a ‘shock’ effect, and sustain this shock effect on the Leydig cells of the testes for a sustained period of the first 1 – 2 weeks of post cycle therapy. Studies have in fact demonstrated the incredible effectiveness of HCG for this purpose, and it is even suggested clinically that HCG be utilized for the purpose of treating anabolic steroid induced hypogonadism[4]. Following this line of thought, the other two compounds (the SERM and the AI) are to be utilized as supportive compounds for HCG use in this 1 – 2 week period, and after HCG is discontinued early on in PCT, only the SERM is to be used in order to carry along the hormonal recovery process.
In spite of the good news in regards to the ability for HCG to assist in hormonal recovery, there are still two remaining issues to be addressed:
– The fact that HCG causes increased production of aromatase, leading to increased Estrogen levels.
– Following the discontinuation of HCG, the body is left with very little endogenous LH and FSH production due to the exogenous administration of HCG.
Aromatase Inhibitors: Aromasin (Exemestane) Above All Else
The first of the two remaining issues to be addressed will be the fact that HCG will trigger increases in testicular aromatase expression, and result in Estrogen increases in the body. It should also be noted that it will cause an increase in testicular progesterone levels. Estrogen rising is of course undesirable during PCT, as it has already been explained that Estrogen will trigger suppression of endogenous Testosterone production, and there is no doubt that any individual wishes to encounter Estrogenic side effects during PCT either.
Therefore, the option here is to include an aromatase inhibitor. However, there exists a big problem in regards to the other two of the three major aromatase inhibitors (Arimidex and Letrozole). The issue is the fact that in a PCT program that includes the use of SERMs such as Nolvadex and Clomid, which are known as absolutely essential components to a PCT program, Arimidex and Letrozole have direct negative interactions with Nolvadex. The problem here is that Arimidex (or Letrozole) and Nolvadex both directly counteract one another. One study has demonstrated that when Arimidex is utilized with Nolvadex, Nolvadex will decrease blood plasma concentration of Arimidex (as well as Letrozole, another commonly used aromatase inhibitor)[5]. The conclusion here is that the use of Arimidex or Letrozole with Nolvadex together is a very bad idea and may work counterproductively if used together in a PCT protocol. Aromasin completely circumvents this problem, as it has been demonstrated to have no interactions what so ever with Nolvadex, unlike the other two aforementioned aromatase inhibitors. In one study, Aromasin displayed no such reduced effectiveness or any reduced blood plasma levels when utilized with Nolvadex[6].
The other benefit of selecting Aromasin over all other AIs is the fact that Aromasin has demonstrated in several studies to impact cholesterol profiles in a negative manner far less than other aromatase inhibitors have, where in one particular study on cancer patients, 24 weeks of Aromasin (Exemestane) administration held no impact on cholesterol profiles[7]. Some other studies have also demonstrated a nil effect on cholesterol profiles from the use of Aromasin[8]. Although there have also been some studies that have demonstrated a negative effect on cholesterol profiles resultant from Aromasin use, it is evident that there is not as a significant or as a negatively impacting effect from Aromasin on cholesterol as other aromatase inhibitors[9].
Finally, in addition to these benefits from Aromasin, it is very clear that Aromasin holds the ability to increase Testosterone levels in males as demonstrated by studies. For example, one particularly notable study selected 12 healthy young male test subjects, and were administered random Aromasin doses of 25mg and 50mg for a 10 day period, and not only was Estrogen suppressed by a significant amount (38%), but Testosterone levels in the test subjects were observed to have increased by an incredible 60%[10].
Following these details, Aromasin would be the best possible aromatase inhibitor of choice in order to combat the increased aromatase activity caused by HCG. Therefore, Aromasin would then be utilized at a full 25mg daily dose, and only while HCG is utilized. Once HCG is discontinued, Aromasin too should be halted.
The only following issue to cover now is that of stimulating and maintaining proper endogenous LH release so as to carry recovery along until the body can become self-sufficient once again.
ERMs: Nolvadex and Clomid
The question is often asked among the anabolic steroid using community: Clomid or Nolvadex? Which one for PCT?
First of all, the best possible addition to HCG in a PCT protocol is Nolvadex (Tamoxifen Citrate), as studies have demonstrated that HCG and Nolvadex utilized together have exhibited a remarkable synergistic effect in terms of stimulating endogenous Testosterone production, and that Nolvadex will actually work to block the desensitization effect on the Leydig cells of the testes caused by high doses of HCG[11]. This is very important, because just as too little LH secretion for extended periods can cause desensitization to gonadotropins, too much gonadotropin stimulation (in the form of HCG or otherwise) will likewise cause a desensitization effect.
Secondly, Nolvadex on a mg for mg basis is far more effective than Clomid in stimulating endogenous Testosterone production, as well as being a more cost-effective choice than Clomid itself. Studies have demonstrated that 150mg of Clomid (Clomiphene Citrate) administered daily raised endogenous Testosterone levels of 10 healthy males by approximately 150%, while incidentally, 20mg of Nolvadex (Tamoxifen Citrate) daily raised endogenous Testosterone levels by the same amount[12]. It is very evident here that Clomid is very effective for this purpose, but Nolvadex seems to be a more cost-effective choice seeing as though it is more effective than Clomid when compared mg for mg. The benefits of Nolvadex over Clomid do not end there – Clomid, although it does exhibit Estrogen antagonist effects at the pituitary gland like Nolvadex does, actually exhibits Estrogen agonist effects there too[13]. What this means is that Clomid will actually work in varying degrees as an Estrogen at the pituitary gland, triggering the negative feedback loop and reducing the output of Testosterone stimulating gonadotropins (LH and FSH). This is a very serious problem during post cycle therapy, which is a period in which individuals are trying to recover their HPTA function rather than halt it even further. Ideally, one would want a SERM that exhibits almost 100% Estrogen antagonistic effects on the pituitary gland, and Nolvadex is the perfect choice for this.
When it comes to the dosing aspect of Nolvadex, The standard dose for PCT and for stimulating the release of GnRH (Gonadotropin Releasing Hormone), LH, FSH, and ultimately Testosterone is that of a simple Nolvadex dose of 20 – 40mg daily. In all studies involving Nolvadex doses used to stimulate endogenous Testosterone production, only 20 – 40mg daily of Nolvadex was utilized, and it has in fact been shown that doubling the dose to 40mg or any higher will not produce any significant difference in endogenous Testosterone secretion. The only reason why many elect to utilize 40mg daily of Nolvadex for the first 1-2 weeks of a PCT program is for the purpose of achieving optimal peak blood plasma levels quicker so as to ensure HPTA recovery quicker.
T
he Final Layout
The ideal post cycle therapy protocol should then be as follows:
4 – 6 weeks Total PCT time (depending on recovery ability of the individual)
Weeks 1 – 2:
– HCG at 1000iu/E2D
– Aromasin (Exemestane) at 25mg/day
– Nolvadex (Tamoxifen Citrate) at 40mg/day
Weeks 2 – 6:
– Nolvadex (Tamoxifen Citrate) at 20mg/day
Additional Optional Components (Vitamins/Supplements/Compounds) to Aid During PCT
Aside from the main components discussed, there are various other components that are largely optional, but still very effective for hormonal recovery of the HPTA during the post cycle therapy weeks.
Vitamin D (Cholecalciferol): There is plenty of established solid evidence through studies that mega dosing Vitamin D (Cholecalciferol) exhibits a significant effect on increasing Testosterone levels in men and also has a significant ability to suppress SHBG levels in the body. One of the best PCT additions is indeed Vitamin D. There is an overabundance of clinical studies in existence demonstrating that low Vitamin D levels corresponds with a low level of endogenous Testosterone production (particularly in the winter months for obvious reasons). In one study conducted in Austria where about 200 subjects were involved with one group administered 3332iu daily of vitamin D, and a placebo group, results had shown that men with sufficient Vitamin D levels had significantly higher levels of Testosterone and significantly lower levels of SHBG when compared to the D-deficient subjects[14]. Androgen levels and Vitamin D levels are associated in men and reveal a concordant seasonal variation[15]. In various other studies, similar findings were reported where subjects who were administered higher amounts of Vitamin D over time demonstrated vast increases in total Testosterone levels, and decreases in SHBG. Anecdotal evidence of people who have been supplementing with vitamin D and getting regular blood work at their doctors are observing large increases in their total and free testosterone levels approximately 1 – 2 months after supplementing with Vitamin D.
Medical References:
[1] Effect of long-term testosterone enanthate administration on male reproductive function: Clinical evaluation, serum FSH, LH, Testosterone and seminal fluid analysis in normal men. J. Mauss, G. Borsch et al. Acta Endocrinol 78 (1975) 373-84.
[2] “Dangers of Excess Estrogen In the Aging Male”. Faloon, William. Life Extension Magazine, November 2008.
[3] Acute stimulation of aromatization in Leydig cells by human chorionic gonadotropin in vitro. Proc Natl Acad Sci USA 76:4460-3/1979.
[4] Anabolic steroid induced hypogonadism treated with human chorionic gonadotropin. Gill GV. Postgrad Med J. 1998 Jan;74(867):45-6.
[5] Comparative clinical pharmacology and pharmacokinetic interactions of aromatase inhibitors. Boeddinghaus IM, Dowsett M. J Steroid Biochem Mol Biol. 2001 Dec;79(1-5):85-91.
[6] Inhibitory effect of combined treatment with the aromatase inhibitor exemestane and tamoxifen on DMBA-induced mammary tumors in rats. Zaccheo T, Giudici D, Di Salle E. J Steroid Biochem Mol Biol. 1993 Mar;44(4-6):677-80.
[7] No adverse impact on serum lipids of the irreversible aromatase inactivator Aromasin [Exemestane (E)] in first-line treatment of metastatic breast cancer (MBC): companion study to a European Organization of Research and Treatment of Cancer (Breast Group) Trial with Pharmacia Upjohn. Lohrisch C., Paridaens R., Dirix L. Y., Beex M., Nooij M., Cameron D. Proc. Am. Soc. Clin. Oncol., 20: 43a 2001.
[8] Pharmacokinetics and dose finding of a potent aromatase inhibitor, aromasin (exemestane), in young males. Mauras N, Lima J, Patel D, Rini A, di Salle E, Kwok A, Lippe B. J Clin Endocrinol Metab. 2003 Dec;88(12):5951-6.
[9] Plasma changes in breast cancer patients during endocrine therapy: lipid measurements and nuclear magnetic resonance (NMR) spectroscopy. Engan T., Krane J., Johannessen D. C., Kvinnsland S. Breast Cancer Res. Treat., 36: 287-297, 1995.
[10] Pharmacokinetics and dose finding of a potent aromatase inhibitor, aromasin (exemestane), in young males. Mauras N, Lima J, Patel D, Rini A, di Salle E, Kwok A, Lippe B. J Clin Endocrinol Metab. 2003 Dec;88(12):5951-6.
[11] Tamoxifen suppresses gonadotropin-induced 17 alpha-hydroxyprogesterone accumulation in normal men. Smals AG, Pieters GF, Drayer JI, Boers GH, Benraad TJ, Kloppenborg PW. J Clin Endocrinol Metab. 1980 Nov;51(5):1026-9.
[12] Hormonal effects of an antiestrogen, tamoxifen, in normal and oligospermic men. Vermeulen A, Comhaire F. Fertil Steril. 1978 Mar;29(3):320-7.
[13] Disparate effect of clomiphene and tamoxifen on pituitary gonadotropin release in vitro. Adashi EY, Hsueh AJ, Bambino TH, Yen SS. Am J Physiol 1981 Feb;240(2):E125-30
[14] Effect of vitamin D supplementation on testosterone levels in men. Pilz S, Frisch S, Koertke H, Kuhn J, Dreier J, Obermayer-Pietsch B, Wehr E, Zittermann A. Horm Metab Res. 2011 Mar;43(3):223-5. doi: 10.1055/s-0030-1269854. Epub 2010 Dec 10.
[15] Association of vitamin D status with serum androgen levels in men. Wehr E, Pilz S, Boehm BO, März W, Obermayer-Pietsch B. Department of Internal Medicine, Division of Endocrinology and Nuclear Medicine, Medical University Graz, Graz, Austria. 2010 Aug;73(2):243-8
Last edited:
