When I first started getting into bodybuilding and learning about pharmacology, a strategy I would see commonly advised on forums and by industry gurus was switching compounds at week 6 or week 8 to avoid androgen receptor downregulation and circumvent a plateau on a steroid cycle.
This strategy is still used just as commonly today.
Basically, the hypothesis was that you should be switching steroids every 6-8 weeks, or else your body gets used to them and they will stop working.
At the time, this made complete sense to me.
Logically you would think that if you use a steroid your body will eventually get used to it and then you will have to switch steroids to keep your body guessing.
Almost like muscle confusion.
An example of a “good” bulking cycle based on this widespread belief will commonly look something like this:
| Testosterone Enanthate | Nandrolone Decanoate | Trenbolone Enanthate | |
| Week 1-8 | 500 mg | 400 mg | |
| Week 1-16 | 500 mg | 400 mg |
At week 8, according to bro-science, your body is now too used to the Deca and switching compounds to something like Trenbolone is necessary to continue growing at the same pace.
Besides the fact that the Deca is actually going to be in your system anyways occupying androgen receptors for months past the point of switching compounds, objectively to many newbies learning about this stuff for the first time, this cycle might look good.
Over the years as I’ve done more research, I’ve started to realize how ridiculous this bro science switching compounds theory is.
It actually gets under my skin that somebody didn’t publicly come out with the truth dispelling this myth sooner, as it would have prevented me from using compounds with far less favorable side effect profiles that I didn’t even need to use to achieve my goals.
All Steroids Basically Do The Same Thing
Androgen receptor activation is accomplished via the same mechanism of action by any steroid (more or less).
Steroids bind to the androgen receptor and transcribe anabolic and androgenic effects in tissues in the body.
Interestingly enough, the human body generally responds in almost the same way to any anabolic steroid, as they all more or less do the same thing at the end of the day.
“After 1935 the best method of discovering and measuring the protein-building action of androgenic steroids in humans proved to be metabolic balance studies.
In 1955, when anabolic steroids with less androgens were developed, the nitrogen-balance method was used again to evaluate and compare the nitrogen-sparing effect of the various preparations.
The findings of the numerous balance studies that were performed are as follows: The injectable 17 beta-esters, such as nandrolone phenylpropionate, nandrolone decanoate and methenolone enanthate exert a strong anabolic action for several weeks, amounting to 2-2.50 g nitrogen/day, which corresponds to a daily gain of 12-15 g protein or 60-75 g lean body mass.
The orally active 17-alkyl derivatives induce a dose-dependent nitrogen-saving effect of the same order.”
Nitrogen retention and protein accretion were roughly the same between all of the steroids evaluated in the study above, which are all compounds commonly switched in and out of cycles nowadays [R].
Some steroids are more tissue selective, some will antagonize SHBG and/or Estrogen more than others, some will result in a dryer cosmetic look that differs from another, but when it comes to lean muscle growth, they all more or less do the same thing in a nitrogen retention context.
Considering this, it would be wise to choose the most well tolerated anabolic agents with the lowest risk profile you can to accomplish your bodybuilding goals.
If nitrogen sparing is more or less the same between two compounds, but one has far less clinical data backing its safety profile and tolerability, why is it that so many guys are reaching for the highest risk compounds they can whenever given the opportunity?
It is not uncommon nowadays to see bros reach for something like DHB (Dihydroboldenone) instead of Nandrolone because of the exotic appeal, and they heard a couple bros on the forums say that it is “like Tren without the side effects.”
Use something with zero data on humans and had sh*t results in the one preclinical rodent model published on it, or use something with lots of clinical data that has proven for years to be one of the most well tolerated mass building agents we can deploy?
I’m sure you can figure out what the logical choice is here.
Androgen Receptors Upregulate In the Presence Of Androgens, Not Downregulate
Switching compounds at week 8 is done to avoid a potential plateau on a steroid cycle by circumventing the supposed androgen receptor downregulation that occurs after a couple months on the same steroid.
The fact is that the complete opposite occurs.
Androgen receptors upregulate in the presence of androgens, not downregulate.
Androgens facilitate their anabolic effects in tissues through their action on multiple cellular targets.
Testosterone increases satellite cell replication and activation, the number of myonuclei, and increases protein accretion.
The myogenic effects on cellular differentiation, proliferation, and muscle protein turnover are accomplished through multiple signaling pathways via the androgen receptor.
Androgen receptors, in the satellite cell as well as several other muscle cell types, are upregulated by androgens [R, R].
We’ve known this since the 80’s [R].
If androgen receptors don’t downregulate with steroid use, then what is causing muscle growth to slow down and plateau?
The main factor that appears to play a role in muscle growth inhibition is the elevation of a protein in the body called Myostatin.
How Myostatin Inhibits Muscle Growth
Myostatin is a protein in the body that acts as a regulator of skeletal muscle mass, limiting how much muscle the body can grow [R].
Examples of Myostatin deficiencies are found in lab based rodent models, as well as in the farming industry with Myostatin deficient cattle.
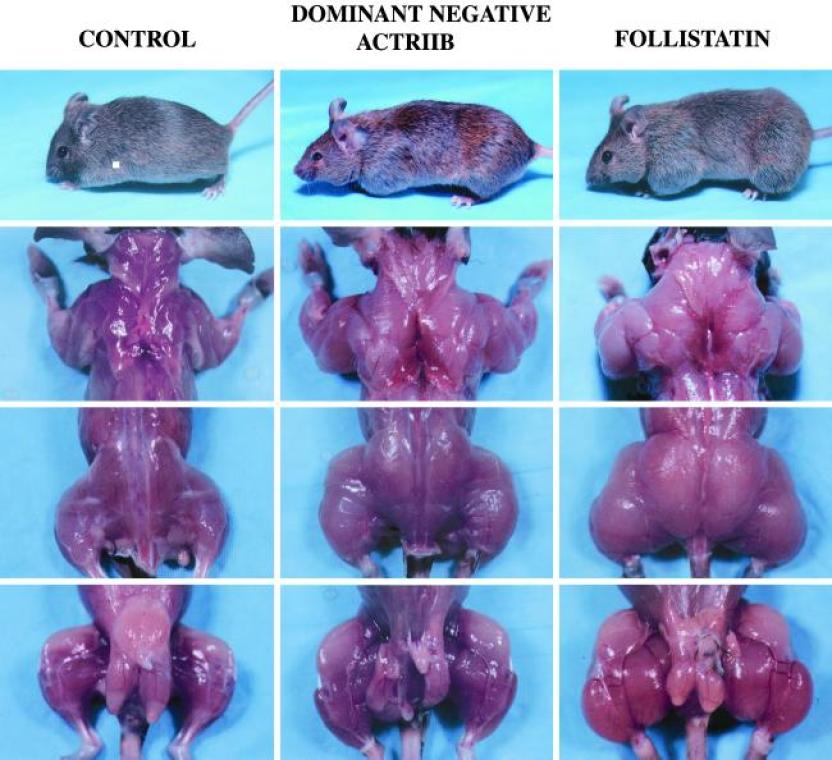
Myostatin Knockout Mice
Mice that lack the gene that creates Myostatin have approximately twice as much muscle mass as normal mice [R].

Belgian Blue Double-Muscled Cattle
The Belgian Blue has a Myostatin gene mutation, consequently preventing its feedback loop of muscle growth inhibition from working correctly.
This mutation interferes with fat deposition and can lead to accelerated lean muscle growth.
The acceleration of muscle growth in Belgian Blues is due primarily to physiological changes in the animal’s muscle cells (fibers) from hypertrophy to a hyperplasia mode of growth.
This growth occurs in the fetus and results in a calf being born with two times the number of muscle fibers as a calf without a Myostatin gene mutation [R].


Myostatin Elevates In Response To Androgens
While there are likely other counterregulatory mechanisms in the body that inhibit excessive muscle growth, the main factor appears to be Myostatin elevation.
Your body doesn’t experience androgen receptor downregulation by week 8 that would then make switching compounds necessary, rather, Myostatin elevates in response to supraphysiological amounts of exogenous androgens and inhibits muscle growth, regardless of what compound is being used.
Switching from NPP to EQ at week 8 will change absolutely nothing when it comes to androgen receptor sensitivity and breaking a plateau.
Myostatin increases to prevent you from gaining unhealthy amounts of muscle.
When you take your Testosterone replacement therapy and your Testosterone binds to androgen receptors, do you eventually have to increase your dose of Testosterone or cycle off of Testosterone to make your TRT work again?
Of course not.
Just like you don’t need to cycle off of your own balls producing Testosterone, because they bind to the androgen receptor in exactly the same way and do not downregulate it.
The only thing that downregulates is your ability to accrue muscle mass in response to androgen receptor activation because of the elevation of inhibiting mechanisms in your body, namely Myostatin.
When you hit week 8 of a cycle and Myostatin is elevated because of your use of supraphysiological amounts of androgens, your body is trying to prevent you from gaining an unhealthy amount of muscle.
This is why you plateau on a cycle, not because the steroid you are using just stops working.
In the following study, the effects of exogenous Testosterone and Trenbolone on Myostatin levels was evaluated [R].
This study showed that after 29 days of administration of either Testosterone or Trenbolone, Myostatin protein levels were 197% higher in the castrated and Testosterone group, and 209% higher in the castrated and Trenbolone group when compared to the placebo.


There’s a reason why this mechanism is in place in our bodies and we can’t grow linearly.
Too much of anything is not going to be good, and when you try to push your body to a place that isn’t healthy, homeostatic mechanisms in the body will try to stop you.
The human body is a big balancing act.
More Androgens = More Myostatin = More Muscle Growth Inhibition
As previously outlined, Myostatin is a growth inhibitor that elevates in the presence of androgens.
Based on the current research it appears that the higher your dose of exogenous anabolics, the greater muscle growth potential you have, and consequently the higher your Myostatin will elevate in parallel to inhibit absurd rates of muscle growth.
In a study evaluating the effect graded doses of Testosterone have on Myostatin levels in young and older men, Myostatin levels were significantly higher on day 56 than baseline in both groups [R].

 The Myostatin hypothesis isn’t air tight and has some holes in the data contradicting its muscle growth inhibiting effects.
The Myostatin hypothesis isn’t air tight and has some holes in the data contradicting its muscle growth inhibiting effects.
However, based on what we know to date, the research suggests that its more than likely the main regulatory mechanism involved in muscle growth response relative to androgen receptor activation.
Myostatin is well known to negatively regulate muscle mass in mice, cattle, dogs and humans [R].
Why Switching Compounds To Deal With “Downregulation” Is A Bad Idea
Switching compounds to break through your plateau will make no difference on your outcomes.
At the end of the day, Myostatin will elevate relative to the anabolic stimulus in the body.
Increase your Testosterone more, Myostatin will elevate.
Switch from Primobolan to Masteron at week 8 and what will happen?
Nothing, androgen receptors are already upregulated and sensitive enough to do what they are supposed to do, but Myostatin will remain elevated regardless of what compounds you switch in and out.
If you experience a plateau on a cycle, switching steroids doesn’t circumvent the root of the issue.
If you switch to something stronger, then Myostatin will only increase even more to match this increase in androgen load in the body.
Switching from Nandrolone to Tren, to EQ, and just randomly swapping things in and out has no effect on transcription at the androgen receptor, the only thing that will change is your body’s production of Myostatin relative to your doses and muscle growth potential (and potentially other undiscovered counterregulatory factors as well).
The main problem with switching compounds in this manner is that you could be using a thoroughly studied compound with very good clinical outcomes, high tolerability in humans, and a very favorable safety profile (e.g. Testosterone, Nandrolone, or Primobolan), and then end up switching to a compound with a far less favorable safety profile riddled with side effects just to achieve the same rate of muscle growth you already had achieved with the safer option.
Bodybuilding gurus will tell their clients to switch from Deca to Trenbolone at week 8 in the offseason simply because of this androgen receptor downregulation broscience, and then put their client in a terrible position where they are using a far more risky compound to achieve nearly the same level of nitrogen retention in the body.
I can’t even fathom how many times this has happened now where a bodybuilder will be using thoroughly studied compounds with hordes of clinical data on humans and switch to some obscure, high-risk steroid with nearly identical muscle growth potential based solely on this androgen receptor hypothesis.
I vividly remember all the bulk phases I did in the past where I would hit week 8 and then wonder what I should do.
If you’re using Nandrolone and you get to week 8, what do you swap to?
Switch to another 19-nor?
Or am I going switch to Tren during the offseason because my Nandrolone has “stopped working” at week 8?
This is the kind of information that hordes of clueless coaches are pushing on their clients.
You could be on a strong foundation of androgens with a great efficacy profile and then have your cookie cutter guru come out and tell you that you need to switch to a compound that’s more dangerous and no better at building muscle than what you’re using because the compounds you’re using are “no longer working,” when it just isn’t the case whatsoever.
Remember, these compounds all more or less do the same thing, so doesn’t it make sense to choose the compounds that build the most muscle with the least side effects, and to stick with those as your staples?
Certain compounds that produce a unique cosmetic look of the muscle should be reserved for pre-contest use only in my opinion, as muscle growth can be achieved during a mass building phase with less risky options.
What To Do After You Plateau On A Steroid Cycle And Myostatin Is Elevated
Once you get deep enough into a cycle, you will plateau.
Now that we have established that the proper course of action IS NOT switching compounds to overcome this nonexistent androgen receptor downregulation, what exactly can you do?
You have a few options here.
Increase Your Calorie Intake
This should be the first thing you do.
Every time you plateau, try increasing your calorie intake a tad.
As little as an additional 100-200 calories per day can be enough to get you gaining again.
Do this until you plateau in strength and size gains and the subsequent increase in your calorie intake just results in more body fat gain.
Increase Your Dose
Once you can no longer break muscle growth plateaus by increasing your calorie intake, that is when increasing your dose of exogenous anabolics is a reasonable strategy to deploy.
Taper up your dose SLOWLY.
This means as low as an additional 50-100 mg on top of your current weekly dosage, and that’s only after you have milked all the growth you can out of the last incremental dosage increase.
Just like you taper up your weights in the gym, or your calorie intake in the kitchen, dosages should be titrated up slowly.
After you increase your weekly dosage, milk all you can out of that incremental titration, and then once you plateau with that go back to step 1 and try increasing your calorie intake again.
Rinse and repeat.
Remember, the higher your doses are, the more your body will fight back, so you should milk the most muscle growth out of each incremental increase in your dosages possible before you increase your dosages again.
I wish I had known this before I ever delved into the world of performance enhancing drugs, as I unnecessarily stressed my body out several times using dosages higher than I needed.
How far can you take this strategy?
Well, as far as you want based on your risk tolerance, up to a point.
Anecdotally, most men will experience significantly diminished returns after passing 1500-2000 mg per week of steroids.
Should you ever get this high to begin with?
Probably not unless you are a competitive bodybuilder who has aspirations of becoming an IFBB pro.
When Myostatin and other counterregulatory mechanisms in the body force you into a plateau, all you can do is increase your nutrient intake, or increase your dosages, and then milk that until Myostatin and other inhibiting factors elevate again to match that new level you have imposed on your body.
These regulatory mechanisms will continue to elevate to match your intake, so how far you push this before cleaning out is up to you.
I know some guys who will titrate all the way up to 2 grams of gear per week and 5000+ calories of food per day over the course of several months.
I also know guys who look great who never go over HRT doses of Testosterone.
What you deem overkill will be based on your health markers, risk tolerance, and personal goals.
Go Off Cycle
Eventually you will have to go off cycle to reset Myostatin (or lower your dose down to therapeutic TRT levels if you need to be on HRT).
If you stay on a high dose of AAS for months, you will eventually plateau.
Regardless of how advanced you are or how high your dosages are, once you decide you don’t want to push your body further with additional nutrients or drugs, you will need to go off cycle to lower the inhibiting mechanisms in your body back to baseline.